

Quality of care after acute coronary syndromes in a prospective cohort with reasons for non-prescription of recommended medications
- PMID: 24676282
- PMCID: PMC3968068
- DOI: 10.1371/journal.pone.0093147
Quality of care after acute coronary syndromes in a prospective cohort with reasons for non-prescription of recommended medications
Abstract
Background: Adherence to guidelines is associated with improved outcomes of patients with acute coronary syndrome (ACS). Clinical registries developed to assess quality of care at discharge often do not collect the reasons for non-prescription for proven efficacious preventive medication in Continental Europe. In a prospective cohort of patients hospitalized for an ACS, we aimed at measuring the rate of recommended treatment at discharge, using pre-specified quality indicators recommended in cardiologic guidelines and including systematic collection of reasons for non-prescription for preventive medications.
Methods: In a prospective cohort with 1260 patients hospitalized for ACS, we measured the rate of recommended treatment at discharge in 4 academic centers in Switzerland. Performance measures for medication at discharge were pre-specified according to guidelines, systematically collected for all patients and included in a centralized database.
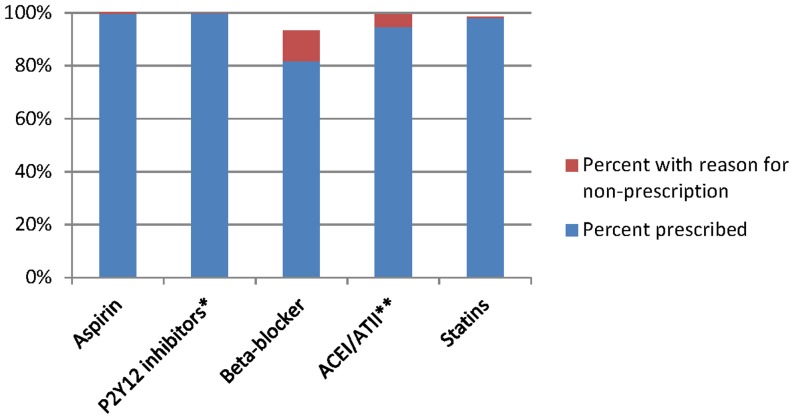
Results: Six hundred and eighty eight patients(54.6%) were discharged with a main diagnosis of STEMI, 491(39%) of NSTEMI and 81(6.4%) of unstable angina. Mean age was 64 years and 21.3% were women. 94.6% were prescribed angiotensin converting enzyme inhibitors/angiotensin II receptor blockers at discharge when only considering raw prescription rates, but increased to 99.5% when including reasons non-prescription. For statins, rates increased from 98% to 98.6% when including reasons for non-prescription and for beta-blockers, from 82% to 93%. For aspirin, rates further increased from 99.4% to 100% and from to 99.8% to 100% for P2Y12 inhibitors.
Conclusions: We found a very high adherence to ACS guidelines for drug prescriptions at discharge when including reasons for non-prescription to drug therapy. For beta-blockers, prescription rates were suboptimal, even after taking into account reason for non-prescription. In an era of improving quality of care to achieve 100% prescription rates at discharge unless contra-indicated, pre-specification of reasons for non-prescription for cardiovascular preventive medication permits to identify remaining gaps in quality of care at discharge.
Trial registration: ClinicalTrials.gov NCT01000701.
Conflict of interest statement
Figures
Similar articles
-
Optimal Medical Therapy Prescription in Patients with Acute Coronary Syndrome in the Netherlands: A Multicenter Pilot Registry.Am J Cardiovasc Drugs. 2021 Mar;21(2):219-229. doi: 10.1007/s40256-020-00427-9. Am J Cardiovasc Drugs. 2021. PMID: 32783182 Free PMC article.
-
Utilization of Evidence-Based Secondary Prevention Medications at the Time of Discharge in Patients with Acute Coronary Syndrome (ACS) in Qatar.Curr Vasc Pharmacol. 2016;14(4):394-403. doi: 10.2174/1570161114666160226150336. Curr Vasc Pharmacol. 2016. PMID: 26916397
-
Age and sex inequalities in the prescription of evidence-based pharmacological therapy following an acute coronary syndrome in Portugal: the EURHOBOP study.Eur J Prev Cardiol. 2014 Nov;21(11):1401-8. doi: 10.1177/2047487313494580. Epub 2013 Jun 20. Eur J Prev Cardiol. 2014. PMID: 23787795
-
[SECONDARY PREVENTION IN PATIENTS WITH ACUTE CORONARY SYNDROME HOSPITALIZED IN INTERNAL MEDICINE DEPARTMENTS].Harefuah. 2015 May;154(5):299-302, 339-40. Harefuah. 2015. PMID: 26168639 Hebrew.
-
Trends in optimal medical therapy at discharge and clinical outcomes in patients with acute coronary syndrome in Thailand.J Cardiol. 2021 Jun;77(6):669-676. doi: 10.1016/j.jjcc.2020.12.015. Epub 2021 Jan 15. J Cardiol. 2021. PMID: 33455848
Cited by
-
Factors influencing harmonized health data collection, sharing and linkage in Denmark and Switzerland: A systematic review.PLoS One. 2019 Dec 12;14(12):e0226015. doi: 10.1371/journal.pone.0226015. eCollection 2019. PLoS One. 2019. PMID: 31830124 Free PMC article.
-
Prognosis of cardiovascular and non-cardiovascular multimorbidity after acute coronary syndrome.PLoS One. 2018 Apr 12;13(4):e0195174. doi: 10.1371/journal.pone.0195174. eCollection 2018. PLoS One. 2018. PMID: 29649323 Free PMC article.
-
Long-Term Quality of Prescription for ST-Segment Elevation Myocardial Infarction (STEMI) Patients: A Real World 1-Year Follow-Up Study.Am J Cardiovasc Drugs. 2020 Feb;20(1):105-115. doi: 10.1007/s40256-019-00361-5. Am J Cardiovasc Drugs. 2020. PMID: 31300969 Free PMC article.
-
Early Discharge in Low-Risk Patients Hospitalized for Acute Coronary Syndromes: Feasibility, Safety and Reasons for Prolonged Length of Stay.PLoS One. 2016 Aug 23;11(8):e0161493. doi: 10.1371/journal.pone.0161493. eCollection 2016. PLoS One. 2016. PMID: 27551861 Free PMC article.
-
The ectopic expression of meiCT genes promotes meiomitosis and may facilitate carcinogenesis.Cell Cycle. 2020 Apr;19(8):837-854. doi: 10.1080/15384101.2020.1743902. Epub 2020 Mar 30. Cell Cycle. 2020. PMID: 32223693 Free PMC article. Review.
References
-
- Butler J, Arbogast PG, BeLue R, Daugherty J, Jain MK, et al. (2002) Outpatient adherence to beta-blocker therapy after acute myocardial infarction. J Am Coll Cardiol 40: 1589–1595. - PubMed
-
- Smith CS, Cannon CP, McCabe CH, Murphy SA, Bentley J, et al. (2005) Early initiation of lipid-lowering therapy for acute coronary syndromes improves compliance with guideline recommendations: observations from the Orbofiban in Patients with Unstable Coronary Syndromes (OPUS-TIMI 16) trial. Am Heart J 149: 444–450. - PubMed
-
- Setoguchi S, Glynn RJ, Avorn J, Mittleman MA, Levin R, et al. (2008) Improvements in long-term mortality after myocardial infarction and increased use of cardiovascular drugs after discharge: a 10-year trend analysis. J Am Coll Cardiol 51: 1247–1254. - PubMed
-
- HEDIS Health Plan Employer Data and Information Set. Washington, DC: National Committee for Quality Insurance (NCQA) website Available: http://www.ncqa.org/. Accessed 2014 March 6.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
