Human papillomavirus and oropharyngeal cancer, the epidemics, and significance of additional clinical biomarkers for prediction of response to therapy (Review)
- PMID: 24676623
- PMCID: PMC4063535
- DOI: 10.3892/ijo.2014.2355
Human papillomavirus and oropharyngeal cancer, the epidemics, and significance of additional clinical biomarkers for prediction of response to therapy (Review)
Abstract
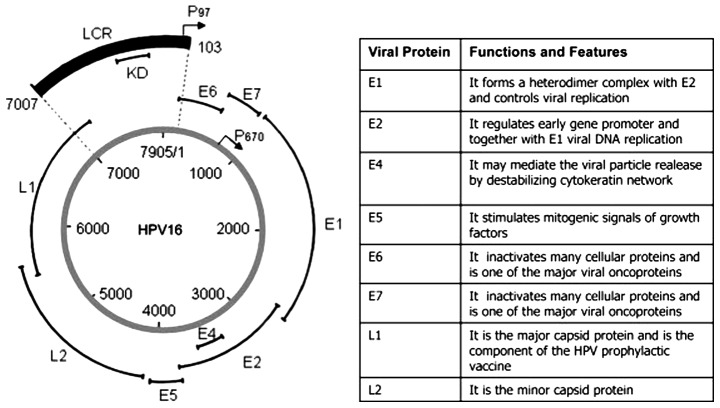
In 2007, the International Agency for Research against Cancer (IARC) recognized human papillomavirus (HPV), especially HPV16, besides smoking and alcohol, as a risk factor for oropharyngeal squamous cell carcinoma (OPSCC), where tonsillar and base of tongue cancer dominate. Moreover, during the past decade, in many Western countries, a sharp rise in the incidence of OPSCC, more specifically of HPV-positive OPSCC has been observed. Notably, patients with HPV-positive OPSCC, where the majority are men, particularly never-smokers have a better clinical outcome than patients with HPV-negative OPSCC and other head neck cancer (roughly 80 vs. 40% disease-free survival with conventional radiotherapy and surgery). This suggests that many patients with HPV-positive OPSCC may not require the more aggressive intensified chemo-radiotherapy given to head neck cancer patients today, and could with somewhat tapered treatment maintain excellent survival, avoiding some of the severe side effects along with intensified treatment. However, before de-intensified treatment is administered additional biomarkers are necessary in combination with HPV-positive status in order to predict and select patients that will respond favorably to therapy. In conclusion, noteworthy issues within this field with an increasing cohort of patients with HPV-positive OPSCC are better-tailored therapy and prevention. Patients with HPV-positive OPSCC, with biomarkers for good response to therapy e.g., low MHC class I, or CD44 expression or high numbers of CD8+ tumor infiltrating lymphocytes, could be included in randomized trials with less severe therapy. Furthermore, possibilities to screen for HPV-positive OPSCC and to vaccinate boys against HPV infection should be further investigated.
Figures
References
-
- Gillison ML, Koch WM, Capone RB, Spafford M, Westra WH, Wu L, Zahurak ML, Daniel RW, Viglione M, Symer DE, Shah KV, Sidransky D. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst. 2000;92:709–720. - PubMed
-
- Mellin H, Friesland S, Lewensohn R, Dalianis T, Munck-Wikland E. Human papillomavirus (HPV) DNA in tonsillar cancer: clinical correlates, risk of relapse, and survival. Int J Cancer. 2000;89:300–304. - PubMed
-
- Dahlstrand HM, Dalianis T. Presence and influence of human papillomaviruses (HPV) in tonsillar cancer. Adv Cancer Res. 2005;93:59–89. - PubMed
-
- WHO . IARC Monographs on the Evaluation of Carcinogenic Risk to Humans. International Agency for Research on Cancer; Lyon: 2007.
-
- Robinson KL, Macfarlane GJ. Oropharyngeal cancer incidence and mortality in Scotland: are rates still increasing? Oral Oncol. 2003;39:31–36. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous