

Comparative analysis of the tissue inflammatory response in human cutaneous and disseminated leishmaniasis
- PMID: 24676653
- PMCID: PMC4015249
- DOI: 10.1590/0074-0276130312
Comparative analysis of the tissue inflammatory response in human cutaneous and disseminated leishmaniasis
Abstract
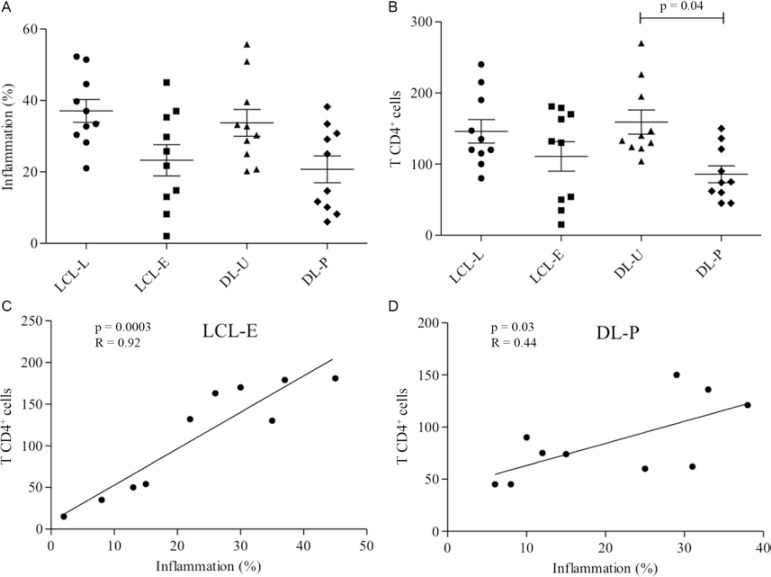
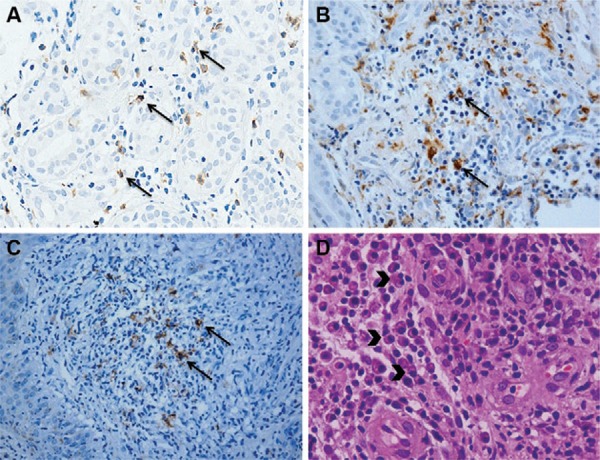
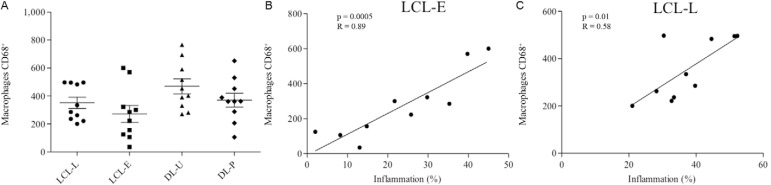
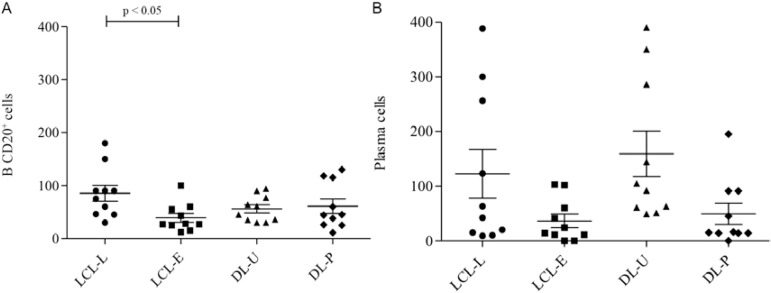
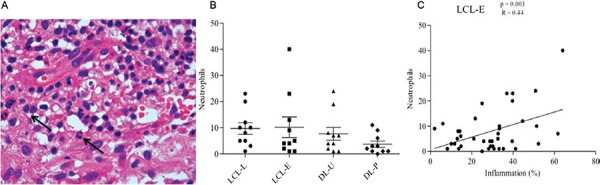
Cutaneous leishmaniasis (CL) is the most frequent clinical form of tegumentary leishmaniasis and is characterised by a single or a few ulcerated skin lesions that may disseminate into multiple ulcers and papules, which characterise disseminated leishmaniasis (DL). In this study, cells were quantified using immunohistochemistry and haematoxylin and eosin staining (CD4+, CD68+, CD20+, plasma cells and neutrophils) and histopathology was used to determine the level of inflammation in biopsies from patients with early CL, late CL and DL (ulcers and papules). The histopathology showed differences in the epidermis between the papules and ulcers from DL. An analysis of the cells present in the tissues showed similarities between the ulcers from localised CL (LCL) and DL. The papules had fewer CD4+ T cells than the DL ulcers. Although both CD4+ cells and macrophages contribute to inflammation in early CL, macrophages are the primary cell type associated with inflammation intensity in late ulcers. The higher frequency of CD20+ cells and plasma cells in lesions demonstrates the importance of B cells in the pathogenesis of leishmaniasis. The number of neutrophils was the same in all of the analysed groups. A comparison between the ulcers from LCL and DL and the early ulcers and papules shows that few differences between these two clinical forms can be distinguished by observing only the tissue.
Figures
References
-
- Afonso L, Borges VM, Cruz H, Ribeiro-Gomes FL, dos Reis G, Dutra AN, Clarêncio J, de Oliveira CI, Barral A, Barral-Netto M, Brodskyn CI. Interactions with apoptotic but not with necrotic neutrophils increase parasite burden in human macrophages infected with Leishmania amazonensis. J Leukoc Biol. 2008;84:389–396. - PubMed
-
- Aga E, Katschinski DM, van Zandbergen G, Laufs H, Hansen B, Müller K, Solbach W, Laskay T. Inhibition of the spontaneous apoptosis of neutrophil granulocytes by the intracellular parasite Leishmania major. J Immunol. 2002;169:898–905. - PubMed
-
- Antonelli LRV, Dutra WO, Almeida RP, Bacellar O, Carvalho EM, Gollob KJ. Activated inflammatory T cells correlate with lesion size in human cutaneous leishmaniasis. Immunol Lett. 2005;101:226–230. - PubMed
-
- Ashford RW, Desjeux P, Deraadt P. Estimation of population at risk of infection and number of cases of leishmaniasis. Parasitol Today. 1992;8:104–105. - PubMed
-
- Azulay RD. Histopatologia da leishmaniose tegumentar. Dermatol Iber Lat Am. 1960;2:7–15.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
