

Quantitative fundus autofluorescence in recessive Stargardt disease
- PMID: 24677105
- PMCID: PMC4008047
- DOI: 10.1167/iovs.13-13624
Quantitative fundus autofluorescence in recessive Stargardt disease
Abstract
Purpose: To quantify fundus autofluorescence (qAF) in patients with recessive Stargardt disease (STGD1).
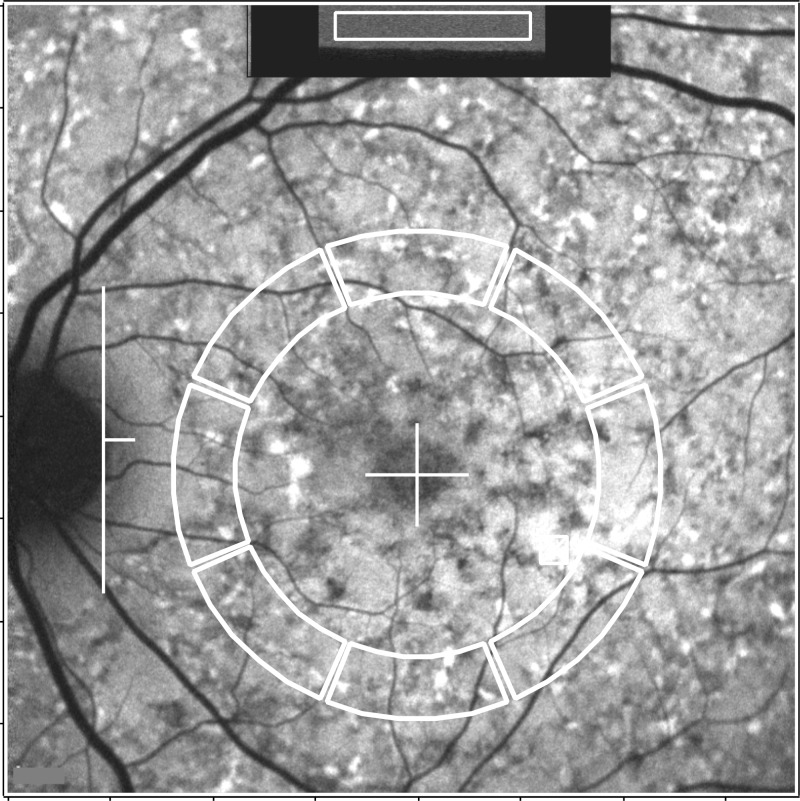
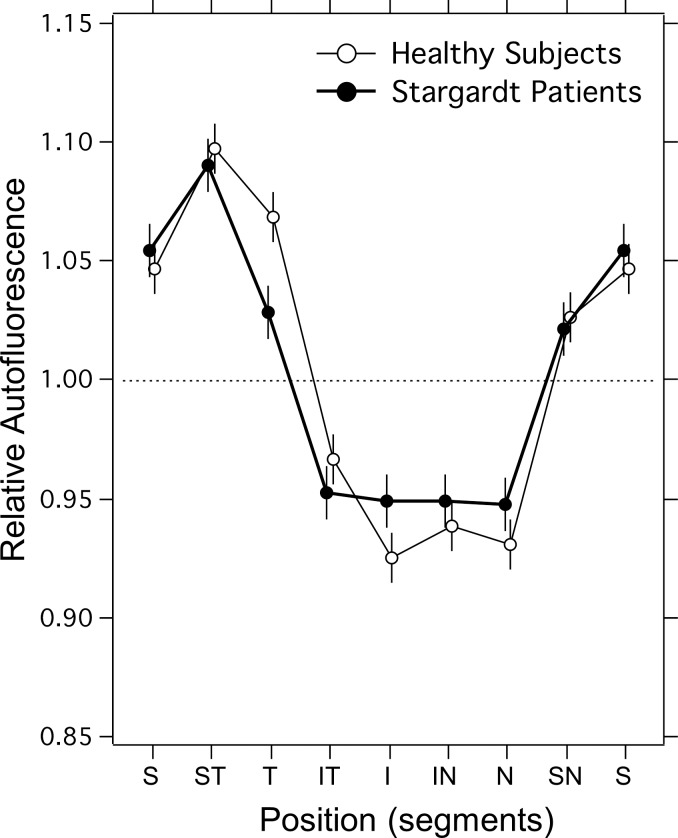
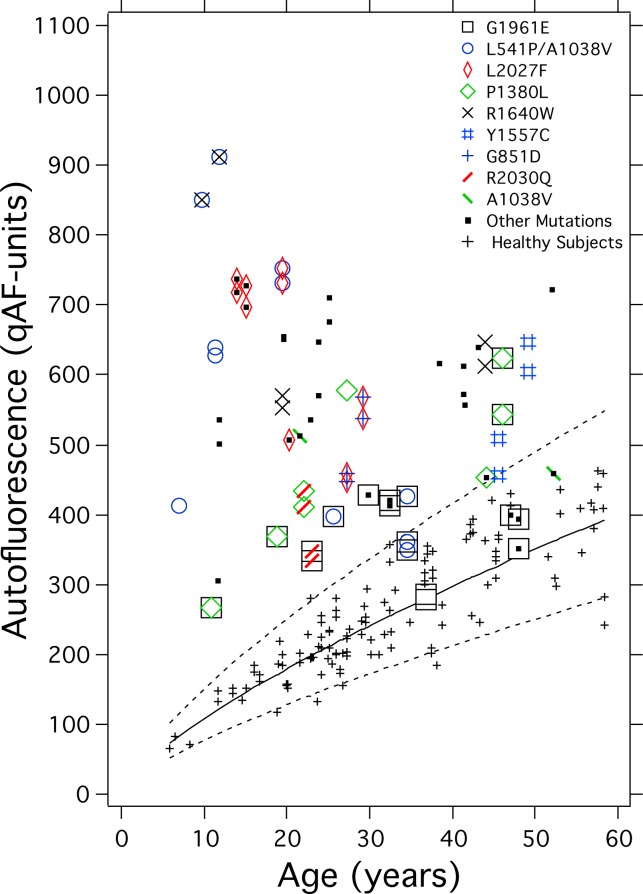
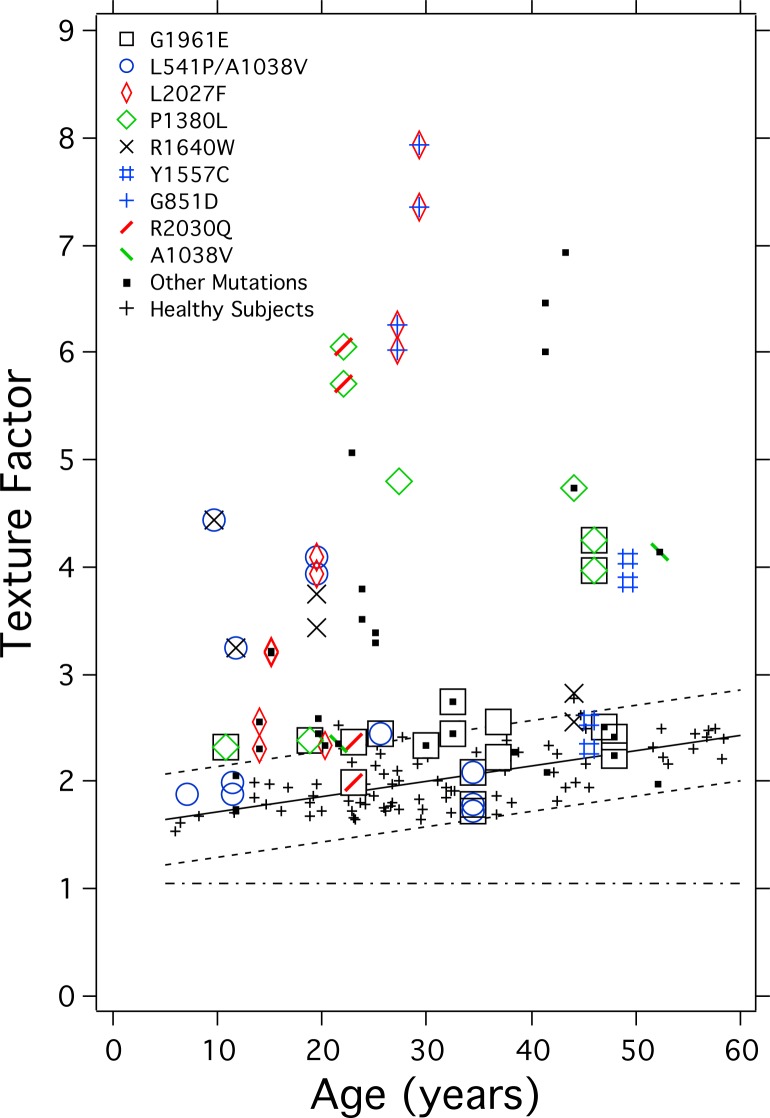
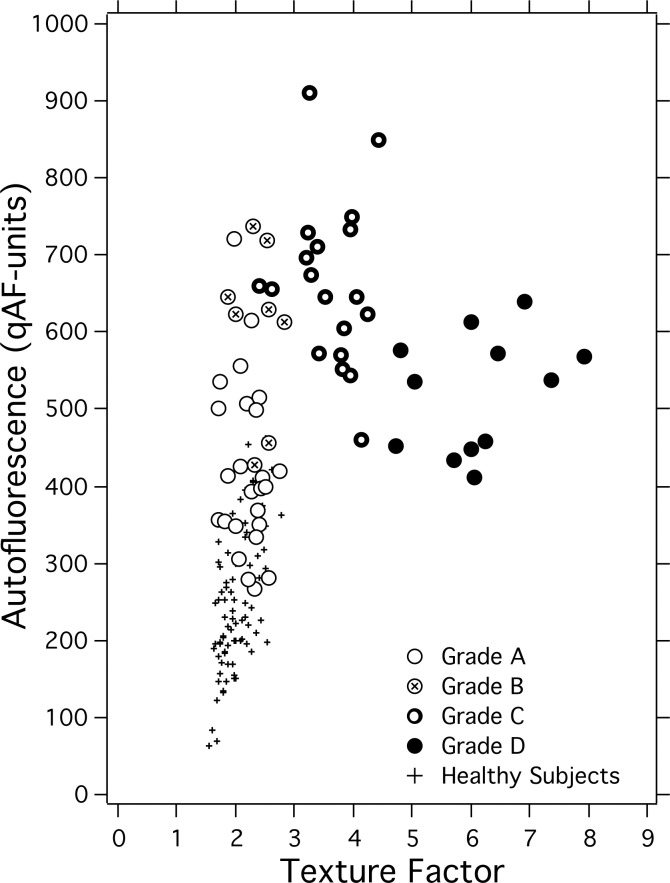
Methods: A total of 42 STGD1 patients (ages: 7-52 years) with at least one confirmed disease-associated ABCA4 mutation were studied. Fundus AF images (488-nm excitation) were acquired with a confocal scanning laser ophthalmoscope equipped with an internal fluorescent reference to account for variable laser power and detector sensitivity. The gray levels (GLs) of each image were calibrated to the reference, zero GL, magnification, and normative optical media density to yield qAF. Texture factor (TF) was calculated to characterize inhomogeneities in the AF image and patients were assigned to the phenotypes of Fishman I through III.
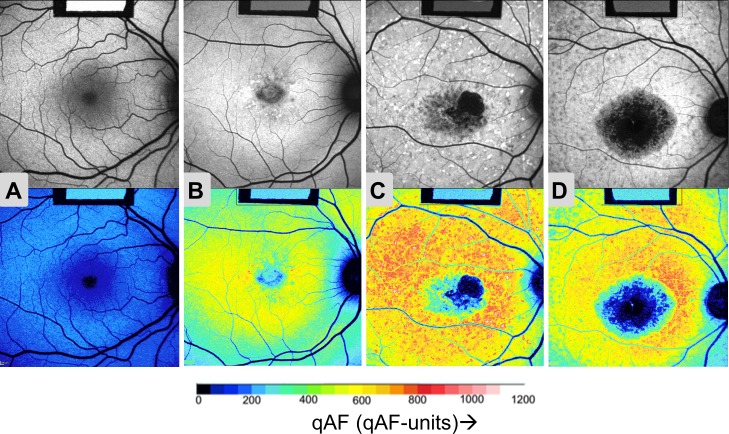
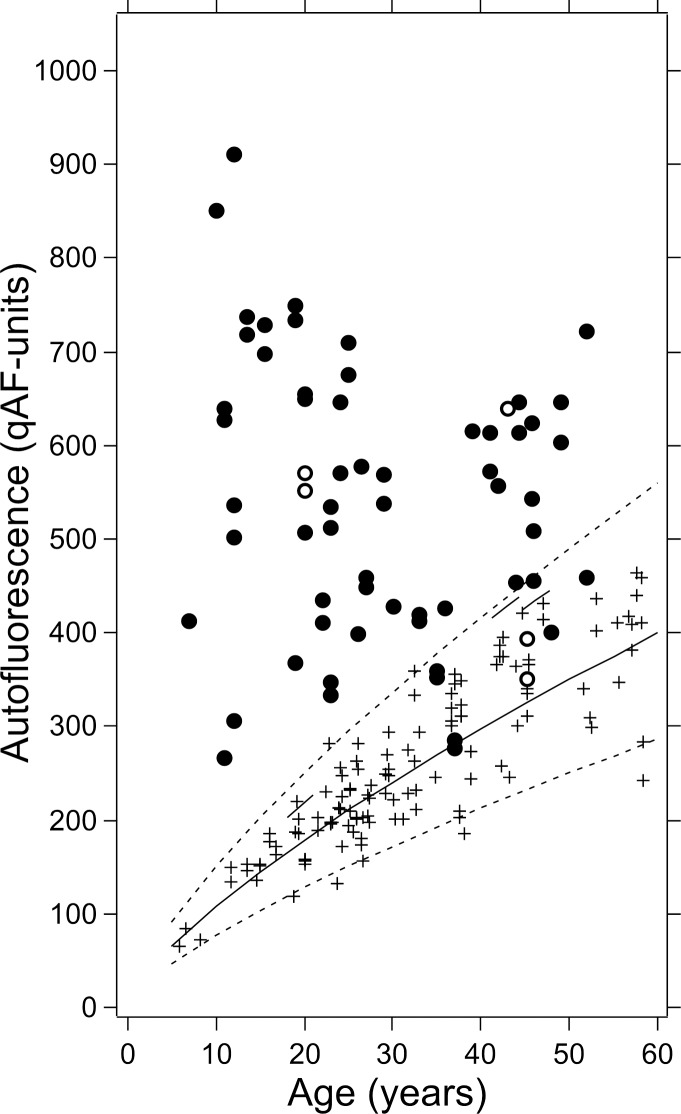
Results: Quantified fundus autofluorescence in 36 of 42 patients and TF in 27 of 42 patients were above normal limits for age. Young patients exhibited the relatively highest qAF, with levels up to 8-fold higher than healthy eyes. Quantified fundus autofluorescence and TF were higher in Fishman II and III than Fishman I, who had higher qAF and TF than healthy eyes. Patients carrying the G1916E mutation had lower qAF and TF than most other patients, even in the presence of a second allele associated with severe disease.
Conclusions: Quantified fundus autofluorescence is an indirect approach to measuring RPE lipofuscin in vivo. We report that ABCA4 mutations cause significantly elevated qAF, consistent with previous reports indicating that increased RPE lipofuscin is a hallmark of STGD1. Even when qualitative differences in fundus AF images are not evident, qAF can elucidate phenotypic variation. Quantified fundus autofluorescence will serve to establish genotype-phenotype correlations and as an outcome measure in clinical trials.
Keywords: ABCA4; lipofuscin; quantitative fundus autofluorescence; recessive Stargardt disease; retinal pigment epithelium; scanning laser ophthalmoscope.
Figures
References
-
- Fishman GA, Farber M, Patel BS, Derlacki DJ. Visual acuity loss in patients with Stargardt's macular dystrophy. Ophthalmology. 1987; 94: 809–814 - PubMed
-
- Rotenstreich Y, Fishman GA, Anderson RJ. Visual acuity loss and clinical observations in a large series of patients with Stargardt disease. Ophthalmology. 2003; 110: 1151–1158 - PubMed
-
- Blacharski PA. Fundus flavimaculatus. In: Newsome DA. ed Retinal Dystrophies and Degenerations. New York: Raven Press; 1988: 135–159
-
- Allikmets R, Singh N, Sun H, et al. A photoreceptor cell-specific ATP-binding transporter gene (ABCR) is mutated in recessive Stargardt macular dystrophy. Nat Genet. 1997; 15: 236–246 - PubMed
-
- Allikmets R, Shroyer NF, Singh N, et al. Mutation of the Stargardt disease gene (ABCR) in age-related macular degeneration. Science. 1997; 277: 1805–1807 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
