

Bone metabolism after bariatric surgery
- PMID: 24677277
- PMCID: PMC4128478
- DOI: 10.1002/jbmr.2226
Bone metabolism after bariatric surgery
Erratum in
-
Re: Bone Metabolism After Bariatric Surgery.J Bone Miner Res. 2018 May;33(5):959. doi: 10.1002/jbmr.3430. Epub 2018 Mar 30. J Bone Miner Res. 2018. PMID: 29727494 No abstract available.
Abstract
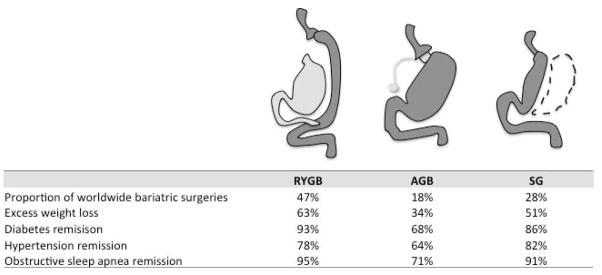
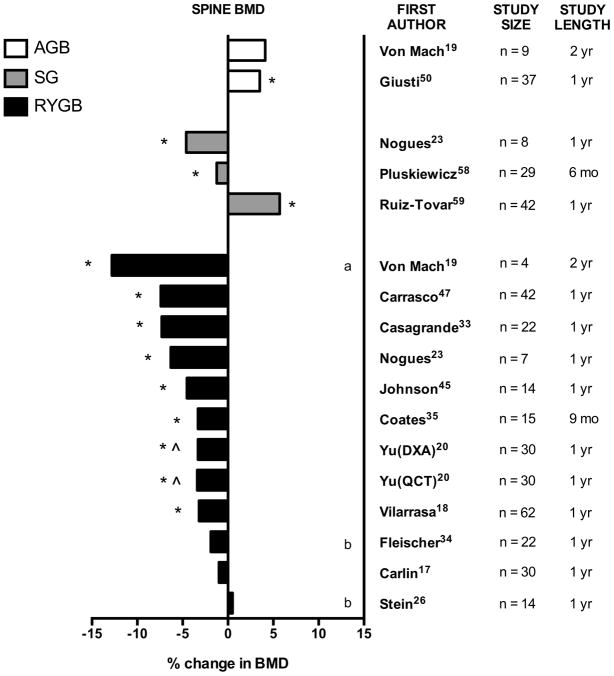
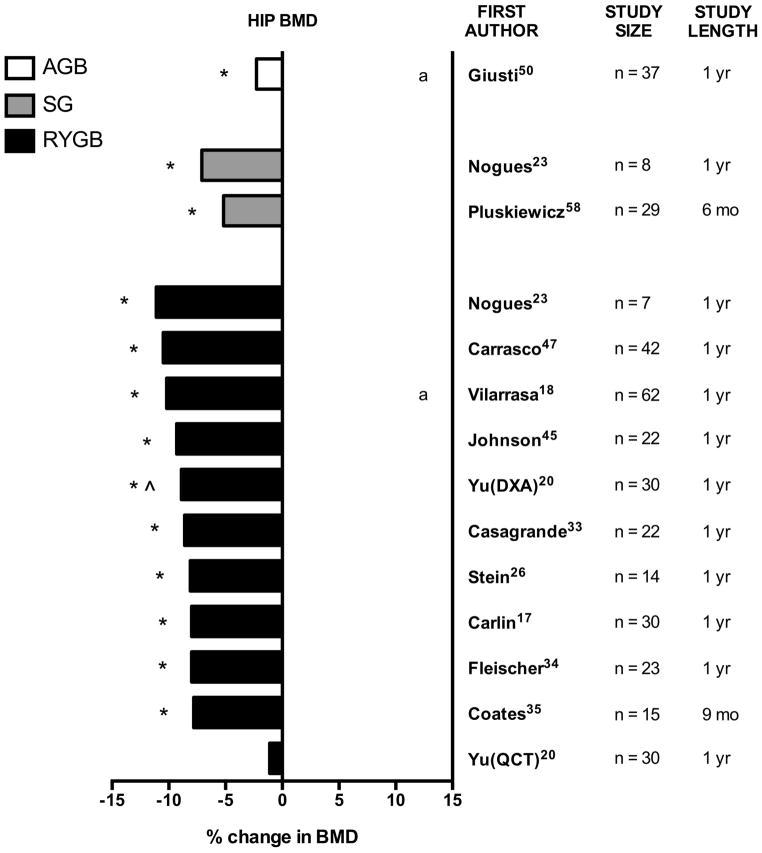
Bariatric surgery is a popular and effective treatment for severe obesity but may have negative effects on the skeleton. This review summarizes changes in bone density and bone metabolism from animal and clinical studies of bariatric surgery, with specific attention to Roux-en-Y gastric bypass (RYGB), adjustable gastric banding (AGB), and sleeve gastrectomy (SG). Skeletal imaging artifacts from obesity and weight loss are also considered. Despite challenges in bone density imaging, the preponderance of evidence suggests that bariatric surgery procedures have negative skeletal effects that persist beyond the first year of surgery, and that these effects vary by surgical type. The long-term clinical implications and current clinical recommendations are presented. Further study is required to determine mechanisms of bone loss after bariatric surgery. Although early studies focused on calcium/vitamin D metabolism and mechanical unloading of the skeleton, it seems likely that surgically induced changes in the hormonal and metabolic profile may be responsible for the skeletal phenotypes observed after bariatric surgery.
Keywords: BARIATRIC SURGERY; BIOCHEMICAL MARKERS OF BONE TURNOVER; DXA; OBESITY.
© 2014 American Society for Bone and Mineral Research.
Figures
References
-
- Sjöström L, Peltonen M, Jacobson P, Sjöström CD, Karason K, Wedel H, et al. Bariatric surgery and long-term cardiovascular events. JAMA: The Journal of the American Medical Association. 2012;307(1):56–65. - PubMed
-
- Fryar CD, Carroll MD, Ogden CL. Prevalence of Overweight, Obesity, and Extreme Obesity Among Adults: United States, Trends 1960–1962 Through 2009–2010 2012. 2014 Jan 5; Available from: http://www.cdc.gov/nchs/data/hestat/obesity_adult_09_10/obesity_adult_09....
-
- Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of Obesity and Trends in the Distribution of Body Mass Index Among US Adults, 1999–2010. JAMA: The Journal of the American Medical Association. 2012 - PubMed
-
- Maggard-Gibbons M, Maglione M, Livhits M, Ewing B, Maher AR, Hu J, et al. Bariatric surgery for weight loss and glycemic control in nonmorbidly obese adults with diabetes: a systematic review. JAMA: The Journal of the American Medical Association. 2013;309(21):2250–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
