

Associations of FGF-23 and sKlotho with cardiovascular outcomes among patients with CKD stages 2-4
- PMID: 24677555
- PMCID: PMC4046724
- DOI: 10.2215/CJN.07870713
Associations of FGF-23 and sKlotho with cardiovascular outcomes among patients with CKD stages 2-4
Abstract
Background and objectives: CKD-mineral and bone disorders (CKD-MBD) measures contribute to cardiovascular morbidity in patients with CKD. Among these, fibroblast growth factor (FGF)-23 and its coreceptor Klotho may exert direct effects on vascular and myocardial tissues. Klotho exists in a membrane-bound and a soluble form (sKlotho). Recent experimental evidence suggests sKlotho has vasculoprotective functions.
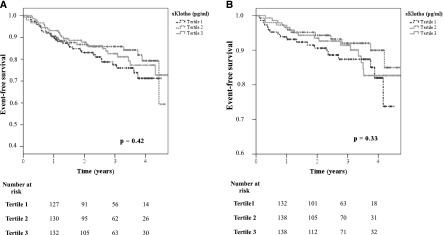
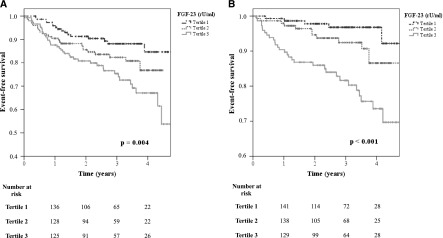
Design, settings, participants, & measurements: Traditional and novel CKD-MBD variables were measured among 444 patients with CKD stages 2-4 recruited between September 2008 and November 2012 into the ongoing CARE FOR HOMe study. Across tertiles of baseline sKlotho and FGF-23, the incidence of two distinct combined end points was analyzed: (1) the first occurrence of an atherosclerotic event or death from any cause and (2) the time until hospital admission for decompensated heart failure or death from any cause.
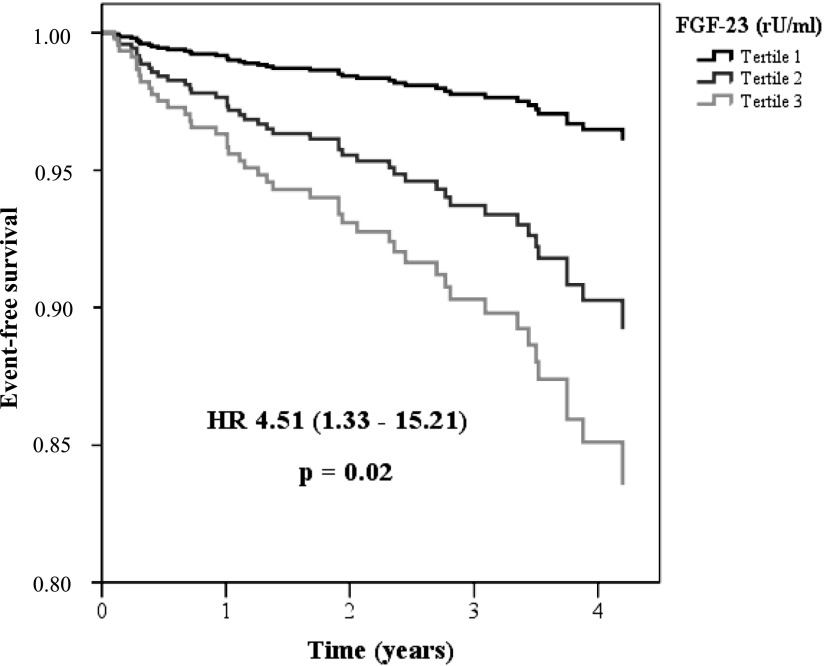
Results: Patients were followed for 2.6 (interquartile range, 1.4-3.6) years. sKlotho tertiles predicted neither atherosclerotic events/death (fully adjusted Cox regression analysis: hazard ratio [HR] for third versus first sKlotho tertile, 0.75 [95% confidence interval (95% CI), 0.43-1.30]; P=0.30) nor the occurrence of decompensated heart failure/death (HR for third versus first sKlotho tertile, 0.81 [95% CI, 0.39-1.66]; P=0.56). In contrast, patients in the highest FGF-23 tertile had higher risk for both end points in univariate analysis. Adjustment for kidney function attenuated the association between FGF-23 and atherosclerotic events/death (HR for third versus first FGF-23 tertile, 1.23 [95% CI, 0.58-2.61]; P=0.59), whereas the association between FGF-23 and decompensated heart failure/death remained significant after adjustment for confounders (HR for third versus first FGF-23 tertile, 4.51 [95% CI, 1.33-15.21]; P=0.02).
Conclusions: In this prospective observational study of limited sample size, sKlotho was not significantly related to cardiovascular outcomes. FGF-23 was significantly associated with future decompensated heart failure but not incident atherosclerotic events.
Keywords: arteriosclerosis; calcium; chronic renal disease; fibroblast.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Herzog CA, Asinger RW, Berger AK, Charytan DM, Díez J, Hart RG, Eckardt KU, Kasiske BL, McCullough PA, Passman RS, DeLoach SS, Pun PH, Ritz E: Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 80: 572–586, 2011 - PubMed
-
- Levin A, Bakris GL, Molitch M, Smulders M, Tian J, Williams LA, Andress DL: Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int 71: 31–38, 2007 - PubMed
-
- Tentori F, Blayney MJ, Albert JM, Gillespie BW, Kerr PG, Bommer J, Young EW, Akizawa T, Akiba T, Pisoni RL, Robinson BM, Port FK: Mortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis 52: 519–530, 2008 - PubMed
-
- Wald R, Sarnak MJ, Tighiouart H, Cheung AK, Levey AS, Eknoyan G, Miskulin DC: Disordered mineral metabolism in hemodialysis patients: An analysis of cumulative effects in the Hemodialysis (HEMO) Study. Am J Kidney Dis 52: 531–540, 2008 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
