

Correlates and variance decomposition analysis of heparin dosing for maintenance hemodialysis in older US patients
- PMID: 24677688
- PMCID: PMC4022350
- DOI: 10.1002/pds.3595
Correlates and variance decomposition analysis of heparin dosing for maintenance hemodialysis in older US patients
Abstract
Purpose: Heparin is commonly used to anticoagulate the hemodialysis (HD) circuit. Despite the bleeding risk, no American standards exist for its administration. We identified correlates and quantified sources of variance in heparin dosing for HD.
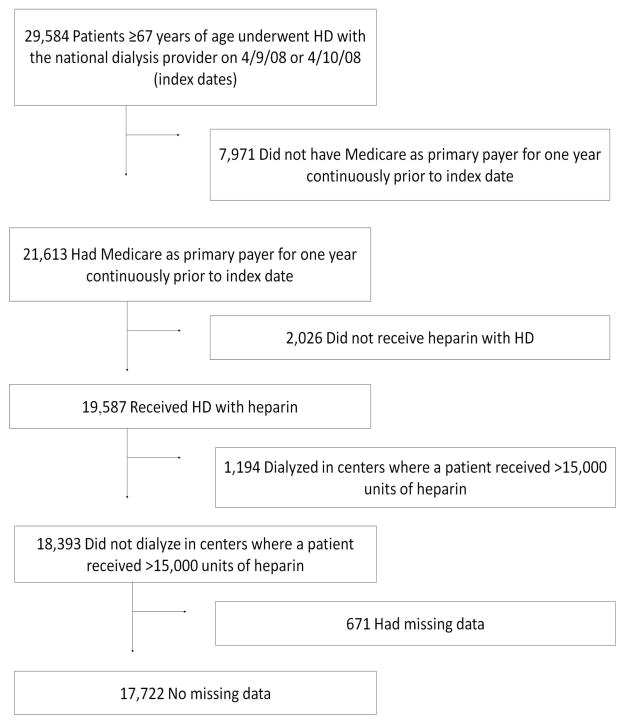
Methods: We performed a cross-sectional study of patients aged 67 years or older who underwent HD with heparin on one of two randomly chosen days in 2008 at a national chain of dialysis facilities. Using a mixed effects model with random intercept for facility and fixed patient and facility characteristics, we examined heparin dosing at patient and facility levels.
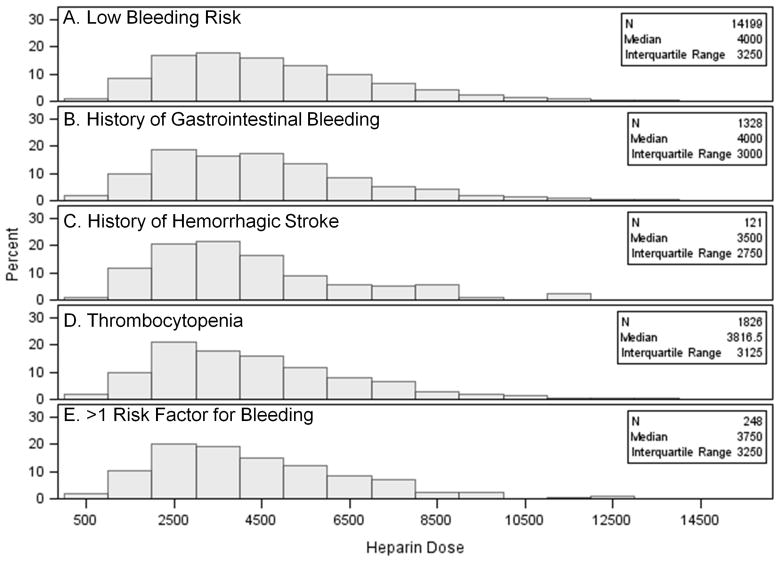
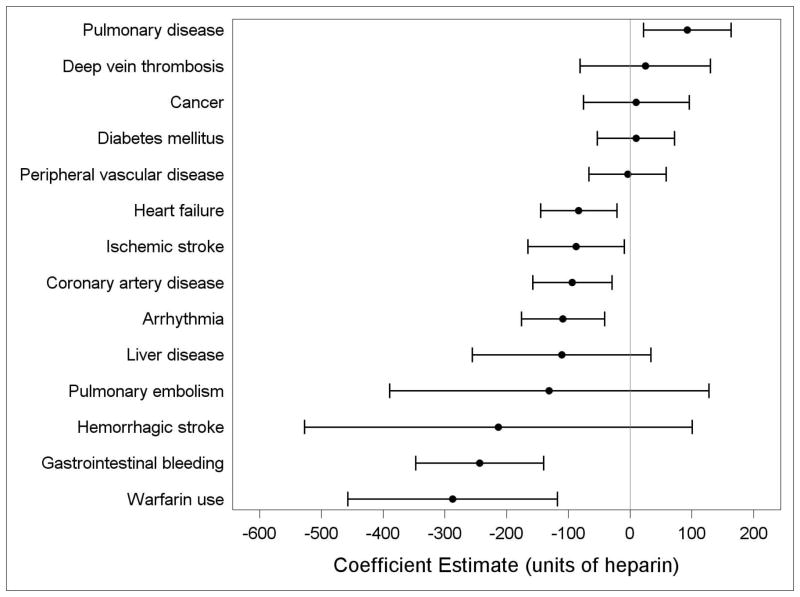
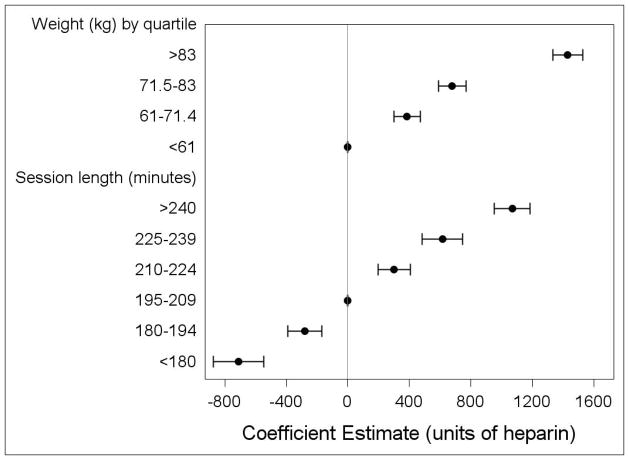
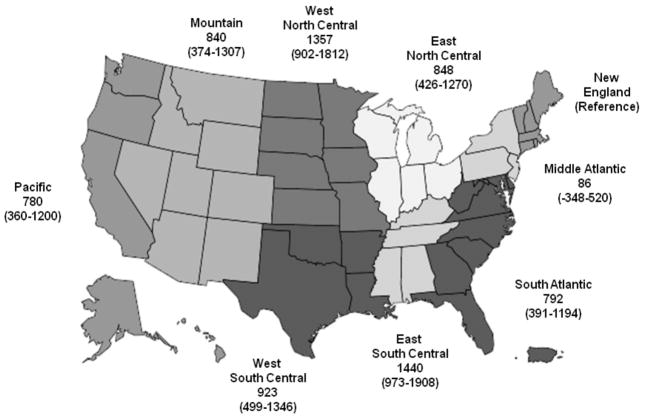
Results: The median heparin dose among the 17 722 patients treated in 1366 facilities was 4000 (25th-75th percentile: 2625-6000) units. In multivariable-adjusted analyses, higher weight, longer session duration, catheter use, and dialyzer reuse were significantly associated with higher heparin dose. Dose also varied considerably among census divisions. Of the overall variance in dose, 21% was due to between-facility differences, independent of facilities' case mix, geography, size, or rurality; 79% was due to differences at the patient level. The patient and facility characteristics in our model explained only 25% of the variance at the patient level.
Conclusions: Despite the lack of standards for heparin administration, we noted patterns of use, including weight-based and time-dependent dosing. Most of the variance was at the patient level; however, only a quarter of it could be explained. The high amount of unexplained variance suggests that factors other than clinical need are driving heparin dosing and that there is likely room for more judicious dosing of heparin.
Keywords: anticoagulation; facility; hemodialysis; heparin; pharmacoepidemiology.
Copyright © 2014 John Wiley & Sons, Ltd.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
