

Autoimmune hemolytic anemia: From lab to bedside
- PMID: 24678166
- PMCID: PMC3943148
- DOI: 10.4103/0973-6247.126681
Autoimmune hemolytic anemia: From lab to bedside
Abstract
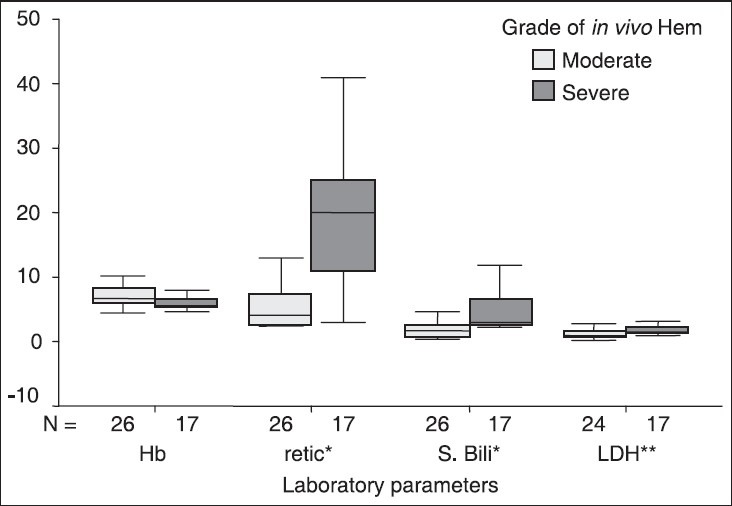
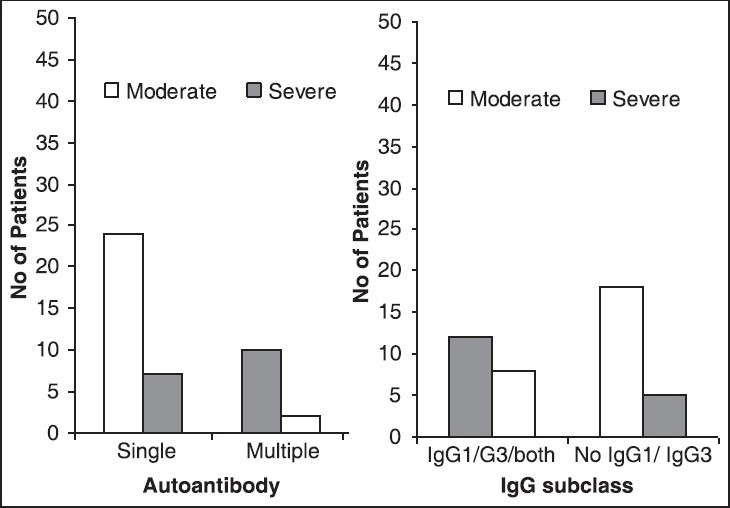
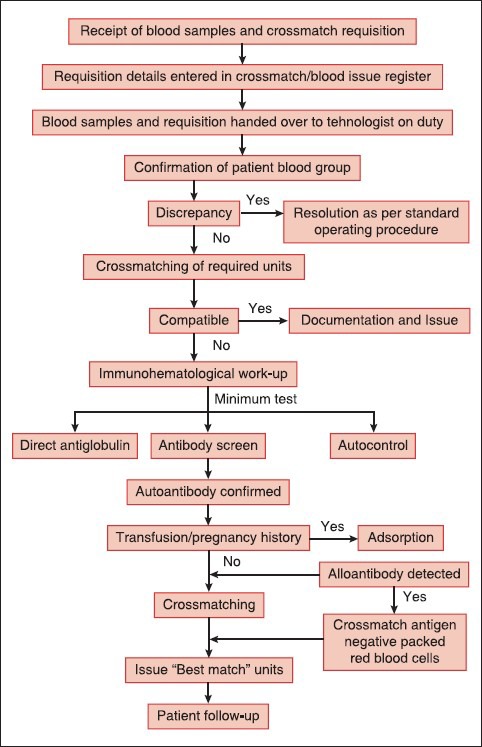
Autoimmune hemolytic anemia (AIHA) is not an uncommon clinical disorder and requires advanced, efficient immunohematological and transfusion support. Many AIHA patients have underlying disorder and therefore, it is incumbent upon the clinician to investigate these patients in detail, as the underlying condition can be of a serious nature such as lymphoproliferative disorder or connective tissue disorder. Despite advances in transfusion medicine, simple immunohematological test such as direct antiglobulin test (DAT) still remains the diagnostic hallmark of AIHA. The sensitive gel technology has enabled the immunohematologist not only to diagnose serologically such patients, but also to characterize red cell bound autoantibodies with regard to their class, subclass and titer in a rapid and simplified way. Detailed characterization of autoantibodies is important, as there is a relationship between in vivo hemolysis and strength of DAT; red cell bound multiple immunoglobulins, immunoglobulin G subclass and titer. Transfusing AIHA patient is a challenge to the immunohematologist as it is encountered with difficulties in ABO grouping and cross matching requiring specialized serological tests such as alloadsorption or autoadsorption. At times, it may be almost impossible to find a fully matched unit to transfuse these patients. However, transfusion should not be withheld in a critically ill patient even in the absence of compatible blood. The "best match" or "least incompatible units" can be transfused to such patients under close supervision without any serious side-effects. All blood banks should have the facilities to perform the necessary investigations required to issue "best match" packed red blood cells in AIHA. Specialized techniques such as elution and adsorption, which at times are helpful in enhancing blood safety in AIHA should be established in all transfusion services.
Keywords: Alloadsorption; alloantibody; autoadsorption; autoantibody; autoimmune hemolytic anemia; best match blood; flow cytometry; gel technology.
Conflict of interest statement
Figures
References
-
- Gehrs BC, Friedberg RC. Autoimmune hemolytic anemia. Am J Hematol. 2002;69:258–71. - PubMed
-
- Duffy TP. Autoimmune hemolytic anemia and paroxysmal nocturnal hemoglobinuria. In: Simon TL, Dzik WH, Synder EL, Stowell CP, Strauss RG, editors. Rossi's Principles of Transfusion Medicine. 3rd ed. Philadelphia, USA: Lippincott Williams and Wilkins Publication; 2002.
-
- Issit P. Serological diagnosis and characterization of causative antibody. In: Chaplin H Jr, editor. Methods in Hematology – Immune Hemolytic Anemia. USA: Churchill Livingston; 1985.
-
- Anderson CL, Looney RJ. Human leukocyte IgG Fc receptors. Immunol Today. 1986;7:264. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
