

Medical therapy of stricturing Crohn's disease: what the gut can learn from other organs - a systematic review
- PMID: 24678903
- PMCID: PMC4230721
- DOI: 10.1186/1755-1536-7-5
Medical therapy of stricturing Crohn's disease: what the gut can learn from other organs - a systematic review
Abstract
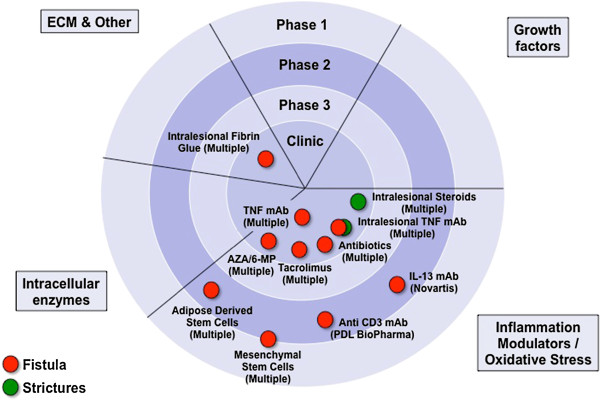
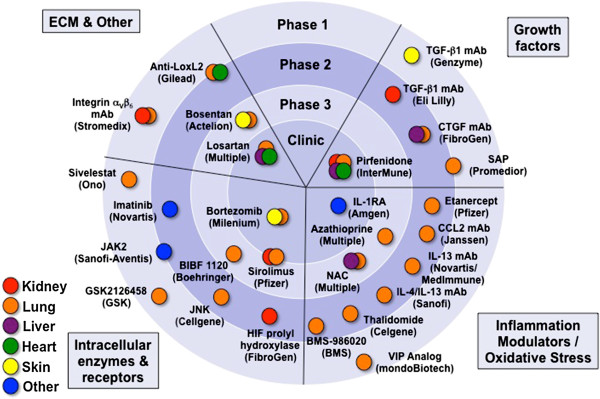
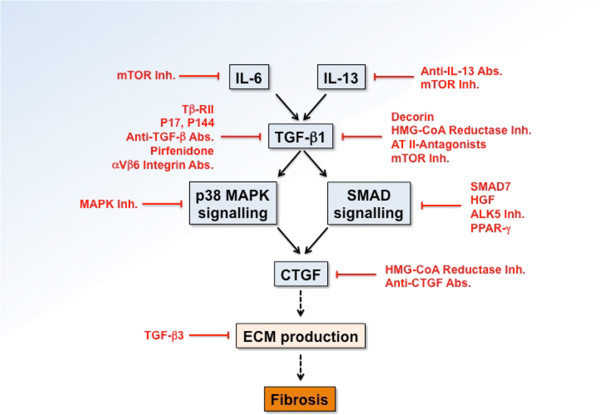
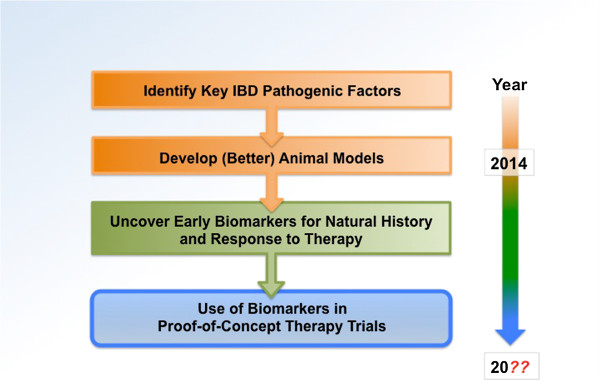
Crohn's disease (CD) is a chronic remitting and relapsing disease. Fibrostenosing complications such as intestinal strictures, stenosis and ultimately obstruction are some of its most common long-term complications. Despite recent advances in the pathophysiological understanding of CD and a significant improvement of anti-inflammatory therapeutics, medical therapy for stricturing CD is still inadequate. No specific anti-fibrotic therapy exists and the incidence rate of strictures has essentially remained unchanged. Therefore, the current therapy of established fibrotic strictures comprises mainly endoscopic dilation as well as surgical approaches. However, these treatment options are associated with major complications as well as high recurrence rates. Thus, a specific anti-fibrotic therapy for CD is urgently needed. Importantly, there is now a growing body of evidence for prevention as well as effective medical treatment of fibrotic diseases of other organs such as the skin, lung, kidney and liver. In face of the similarity of molecular mechanisms of fibrogenesis across these organs, translation of therapeutic approaches from other fibrotic diseases to the intestine appears to be a promising treatment strategy. In particular transforming growth factor beta (TGF-β) neutralization, selective tyrosine kinase inhibitors, blockade of components of the renin-angiotensin system, IL-13 inhibitors and mammalian target of rapamycin (mTOR) inhibitors have emerged as potential drug candidates for anti-fibrotic therapy and may retard progression or even reverse established intestinal fibrosis. However, major challenges have to be overcome in the translation of novel anti-fibrotics into intestinal fibrosis therapy, such as the development of appropriate biomarkers that predict the development and accurately monitor therapeutic responses. Future clinical studies are a prerequisite to evaluate the optimal timing for anti-fibrotic treatment approaches, to elucidate the best routes of application, and to evaluate the potential of drug candidates to reach the ultimate goal: the prevention or reversal of established fibrosis and strictures in CD patients.
Figures
References
-
- Lenze F, Wessling J, Bremer J, Ullerich H, Spieker T, Weckesser M, Gonschorrek S, Kannengiesser K, Rijcken E, Heidemann J, Luegering A, Schober O, Domschke W, Kucharzik T, Maaser C. Detection and differentiation of inflammatory versus fibromatous Crohn’s disease strictures: prospective comparison of 18 F-FDG-PET/CT, MR-enteroclysis, and transabdominal ultrasound versus endoscopic/histologic evaluation. Inflamm Bowel Dis. 2012;18:2252–2260. doi: 10.1002/ibd.22930. - DOI - PubMed
-
- Schoepfer AM, Safroneeva E, Vavricka SR, Peyrin-Biroulet L, Mottet C. Treatment of fibrostenotic and fistulizing Crohn’s disease. Digestion. 2012;86(Suppl 1):23–27. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
