

Bariatric surgery versus intensive medical therapy for diabetes--3-year outcomes
- PMID: 24679060
- PMCID: PMC5451259
- DOI: 10.1056/NEJMoa1401329
Bariatric surgery versus intensive medical therapy for diabetes--3-year outcomes
Abstract
Background: In short-term randomized trials (duration, 1 to 2 years), bariatric surgery has been associated with improvement in type 2 diabetes mellitus.
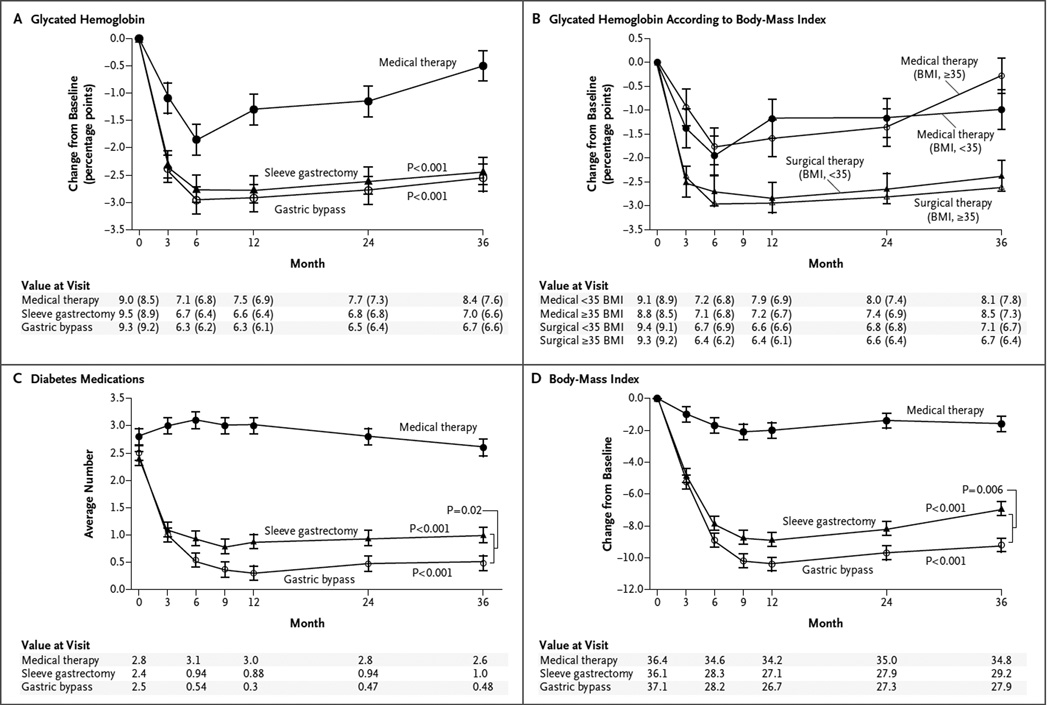
Methods: We assessed outcomes 3 years after the randomization of 150 obese patients with uncontrolled type 2 diabetes to receive either intensive medical therapy alone or intensive medical therapy plus Roux-en-Y gastric bypass or sleeve gastrectomy. The primary end point was a glycated hemoglobin level of 6.0% or less.
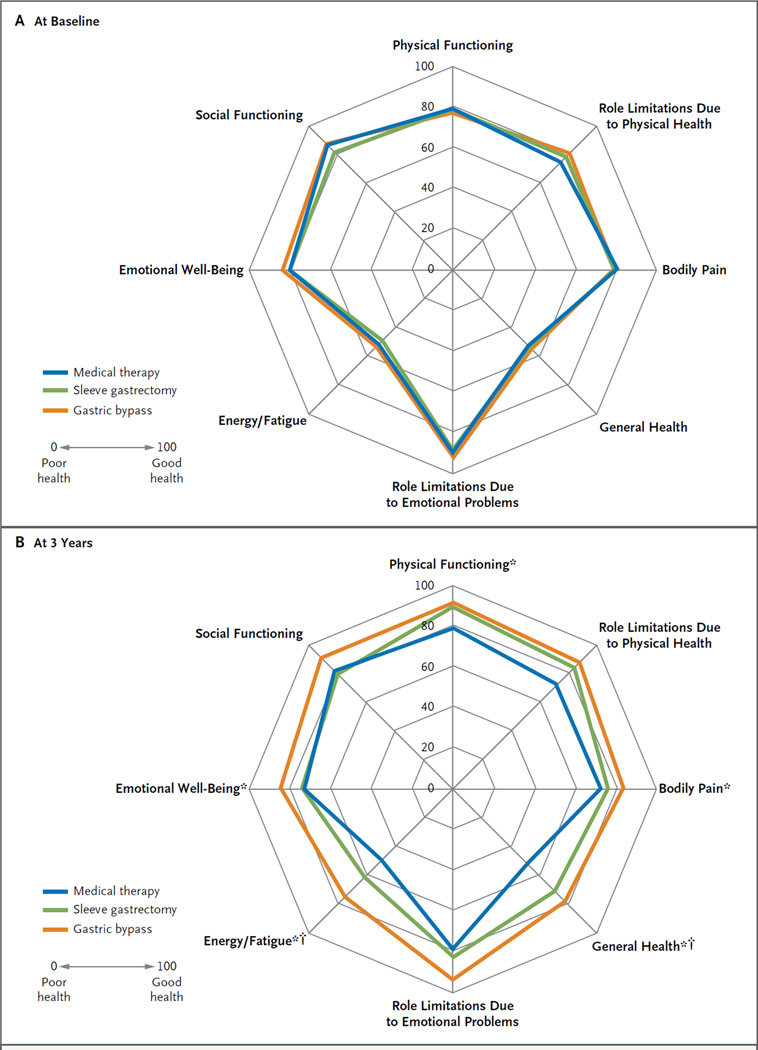
Results: The mean (±SD) age of the patients at baseline was 48±8 years, 68% were women, the mean baseline glycated hemoglobin level was 9.3±1.5%, and the mean baseline body-mass index (the weight in kilograms divided by the square of the height in meters) was 36.0±3.5. A total of 91% of the patients completed 36 months of follow-up. At 3 years, the criterion for the primary end point was met by 5% of the patients in the medical-therapy group, as compared with 38% of those in the gastric-bypass group (P<0.001) and 24% of those in the sleeve-gastrectomy group (P=0.01). The use of glucose-lowering medications, including insulin, was lower in the surgical groups than in the medical-therapy group. Patients in the surgical groups had greater mean percentage reductions in weight from baseline, with reductions of 24.5±9.1% in the gastric-bypass group and 21.1±8.9% in the sleeve-gastrectomy group, as compared with a reduction of 4.2±8.3% in the medical-therapy group (P<0.001 for both comparisons). Quality-of-life measures were significantly better in the two surgical groups than in the medical-therapy group. There were no major late surgical complications.
Conclusions: Among obese patients with uncontrolled type 2 diabetes, 3 years of intensive medical therapy plus bariatric surgery resulted in glycemic control in significantly more patients than did medical therapy alone. Analyses of secondary end points, including body weight, use of glucose-lowering medications, and quality of life, also showed favorable results at 3 years in the surgical groups, as compared with the group receiving medical therapy alone. (Funded by Ethicon and others; STAMPEDE ClinicalTrials.gov number, NCT00432809.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
[Does a gastric bypass improve diabetes control? - Metabolic surgery: success depends on the patient].Dtsch Med Wochenschr. 2014 Aug;139(33):1644. doi: 10.1055/s-0033-1353912. Epub 2014 Aug 5. Dtsch Med Wochenschr. 2014. PMID: 25093949 German. No abstract available.
-
Bariatric surgery versus intensive medical therapy for diabetes.N Engl J Med. 2014 Aug 14;371(7):682. doi: 10.1056/NEJMc1407393. N Engl J Med. 2014. PMID: 25119615 No abstract available.
-
Bariatric surgery versus intensive medical therapy for diabetes.N Engl J Med. 2014 Aug 14;371(7):680. doi: 10.1056/NEJMc1407393. N Engl J Med. 2014. PMID: 25119616 No abstract available.
-
Bariatric surgery versus intensive medical therapy for diabetes.N Engl J Med. 2014 Aug 14;371(7):680-1. doi: 10.1056/NEJMc1407393. N Engl J Med. 2014. PMID: 25119617 No abstract available.
-
Bariatric surgery versus intensive medical therapy for diabetes.N Engl J Med. 2014 Aug 14;371(7):681. doi: 10.1056/NEJMc1407393. N Engl J Med. 2014. PMID: 25119618 No abstract available.
-
Bariatric surgery versus intensive medical therapy for diabetes.N Engl J Med. 2014 Aug 14;371(7):681-2. doi: 10.1056/NEJMc1407393. N Engl J Med. 2014. PMID: 25119619 No abstract available.
-
ACP Journal Club. Bariatric surgery improved HbA1c more than intensive medical therapy in obese patients with uncontrolled type 2 DM.Ann Intern Med. 2014 Aug 19;161(4):JC4. doi: 10.7326/0003-4819-161-4-201408190-02004. Ann Intern Med. 2014. PMID: 25133383 No abstract available.
-
[Bariatric surgery in diabetic patients causes better blood sugar control than drug therapy alone].Praxis (Bern 1994). 2014 Sep 3;103(18):1089-90. doi: 10.1024/1661-8157/a001761. Praxis (Bern 1994). 2014. PMID: 25183619 German. No abstract available.
-
[Bariatric surgery versus intensive treatment in the patient with type 2 diabetes: A follow-up of 3 years].Semergen. 2015 Jan-Feb;41(1):52-3. doi: 10.1016/j.semerg.2014.07.015. Epub 2014 Oct 31. Semergen. 2015. PMID: 25442464 Spanish. No abstract available.
References
-
- Vest AR, Heneghan HM, Agarwal S, Schauer PR, Young JB. Bariatric surgery and cardiovascular outcomes: a systematic review. Heart. 2012;98:1763–1777. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous