

Trends in stroke rates, risk, and outcomes in the United States, 1988 to 2008
- PMID: 24680794
- PMCID: PMC4125206
- DOI: 10.1016/j.amjmed.2014.03.017
Trends in stroke rates, risk, and outcomes in the United States, 1988 to 2008
Abstract
Background: Stroke is a major cause of morbidity and mortality. We describe trends in the incidence, outcomes, and risk factors for stroke in the US Medicare population from 1988 to 2008.
Methods: We analyzed data from a 20% sample of hospitalized Medicare beneficiaries with a principal discharge diagnosis of ischemic (n = 918,124) or hemorrhagic stroke (n = 133,218). Stroke risk factors were determined from the National Health and Nutrition Examination Survey (years 1988-1994, 2001-2008) and medication uptake from the Medicare Current Beneficiary Survey (years 1992-2008). Primary outcomes were stroke incidence and 30-day mortality after stroke hospitalization.
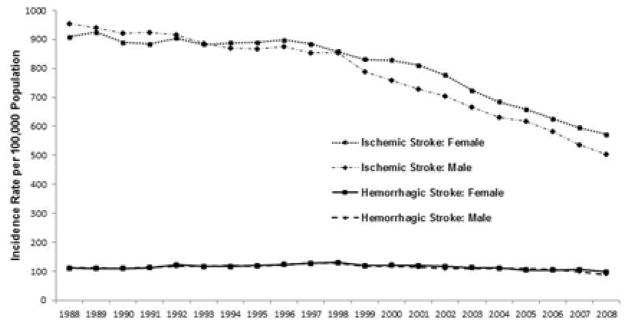
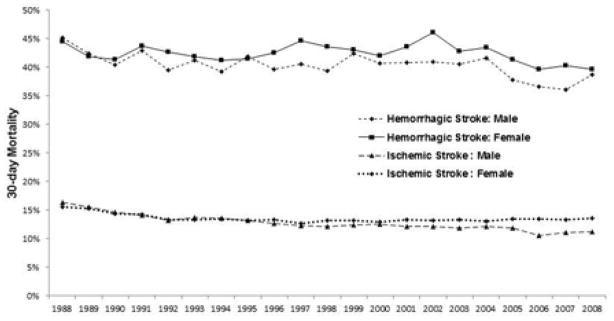
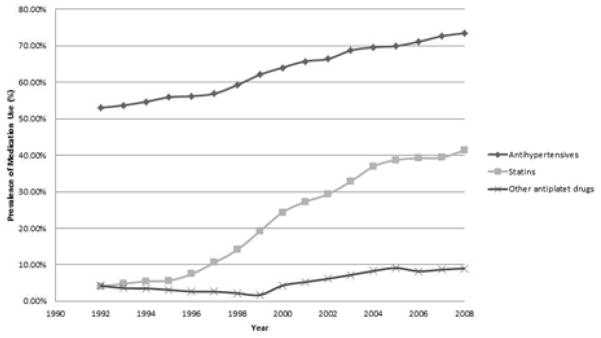
Results: Ischemic stroke incidence decreased from 927 per 100,000 in 1988 to 545 per 100,000 in 2008, and hemorrhagic stroke decreased from 112 per 100,000 to 94 per 100,000. Risk-adjusted 30-day mortality decreased from 15.9% in 1988 to 12.7% in 2008 for ischemic stroke and from 44.7% to 39.3% for hemorrhagic stroke. Although observed stroke rates decreased, the Framingham stroke model actually predicted increased stroke risk (mean stroke score 8.3% in 1988-1994, 8.8% in 2005-2008). Statin use in the general population increased (4.0% in 1992, 41.4% in 2008), as did antihypertensive use (53.0% in 1992, 73.5% in 2008).
Conclusions: Incident strokes in the Medicare population aged ≥65 years decreased by approximately 40% over the last 2 decades, a decline greater than expected on the basis of the population's stroke risk factors. Case fatality from stroke also declined. Although causality cannot be proven, declining stroke rates paralleled increased use of statins and antihypertensive medications.
Keywords: Antihypertensive medications; Hemorrhagic stroke; Ischemic stroke; Mortality; Outcomes; Risk; Statins; Stroke; Trends.
Copyright © 2014 Elsevier Inc. All rights reserved.
Conflict of interest statement
Margaret Fang: study design, data interpretation, drafting results, critical review. No conflicts of interest to disclose. Dr. Fang had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Marcelo Coca Peraillon: data analysis and interpretation, drafting results, critical review. No conflicts of interest to disclose.
Kaushik Ghosh: data analysis and interpretation, drafting results, critical review. No conflicts of interest to disclose.
David Cutler: study design, data interpretation, critical review. No conflicts of interest to disclose.
Allison Rosen: study design, data interpretation, critical review. No conflicts of interest to disclose.
Figures
References
-
- Goldstein LB, Bushnell CD, Adams RJ, Appel LJ, Braun LT, Chaturvedi S, et al. Guidelines for the primary prevention of stroke. Stroke. 2011;42:517–584. - PubMed
-
- Murphy SL, Xu JQ, Kochanek KD. Deaths, preliminary data for 2010. National Vital Statistics Reports. 2012;60:1–68. - PubMed
-
- Psaty BM, Lumley T, Furberg CD, Schellenbaum G, Pahor M, Alderman MH, et al. Health outcomes associated with various antihypertensive therapies used as first-line agents. JAMA: The Journal of the American Medical Association. 2003;289:2534–2544. - PubMed
-
- Amarenco P, Labreuche J, Lavallée P, Touboul P-J. Statins in stroke prevention and carotid atherosclerosis. Stroke. 2004;35:2902–2909. - PubMed
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. Journal of Chronic Disease. 1987;40:373–383. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
