

Effects of newly developed chemotherapy regimens, comorbidities, chemotherapy-related toxicities on the changing patterns of the leading causes of death in elderly patients with colorectal cancer
- PMID: 24681607
- PMCID: PMC4110447
- DOI: 10.1093/annonc/mdu131
Effects of newly developed chemotherapy regimens, comorbidities, chemotherapy-related toxicities on the changing patterns of the leading causes of death in elderly patients with colorectal cancer
Abstract
Background: Abundant evidences have shown that newly developed chemotherapy regimens improved 5-year survival rate of colorectal cancer (CRC) patients over the past two decades. However, their impact on risk of death from leading causes among elderly patients is still poorly understood.
Patients and methods: A retrospective cohort study of 69 718 elderly CRC patients with their first primary tumors in 1992-2009, identified from the 12 areas of Surveillance, Epidemiology, and End Results-Medicare linked database with their Medicare claims up to 2010. Multivariate Cox regression models were used to assess the effect of newly developed chemotherapy regimens, comorbidities, and chemotherapy related toxicities on cause-specific death and their temporal patterns among elderly CRC patients.
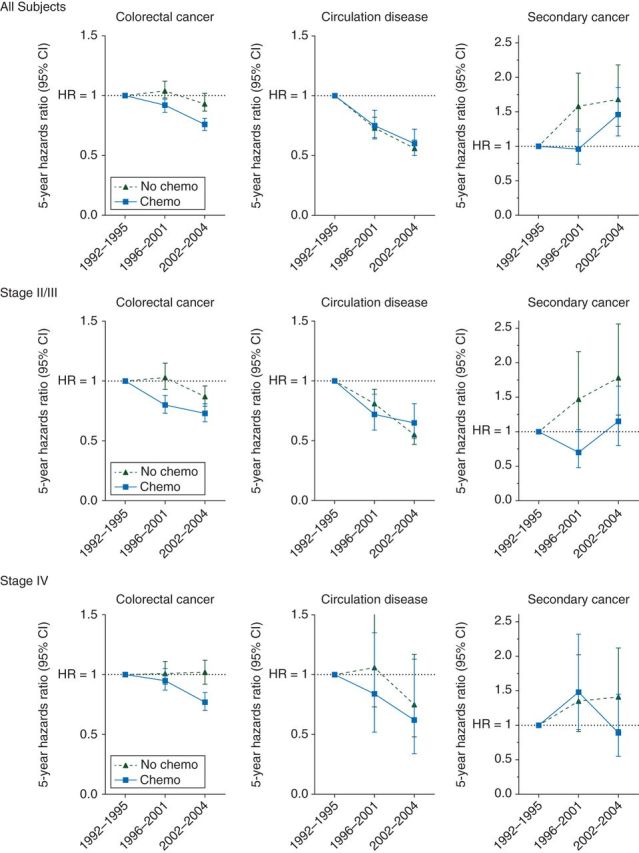
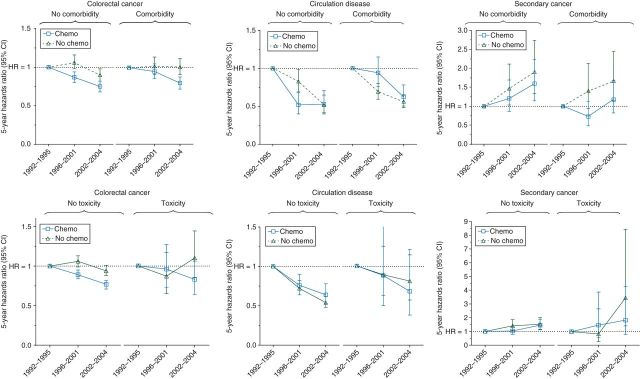
Results: The leading causes of death among CRC patients were CRC, circulation disorders, and secondary cancers, which accounted for 51.4%, 25%, and 4.6% of all-cause death, respectively. Patients diagnosed in more recent diagnostic time periods were significantly less likely to die of CRC [period 2: 5-year hazard ratio = 0.94, 95% confidence interval (CI) 0.90-0.97; period 3: 0.86, 0.83-0.90], circulation disorders (period 2: 0.94, 0.88-1.00; period 3: 0.80, 0.75-0.87), and more likely to die of secondary cancer (period 3: 1.42, 1.20-1.68) compared with those diagnosed in period 1. Charlson comorbidities index and the selected pre-existing comorbidities were significantly associated with increased 5-year risk of death from all three leading causes. Both hematological and gastric toxicity were associated with reduced risk of death from CRC and circulation disorders. The association between diagnostic time period and risk reduction in death from CRC depended on chemotherapy treatment (P < 0.0001). Subgroup analyses showed that the chemotherapy-dependent significant risk reduction was seen in patients with stage II-III CRC, patients without comorbidities, and patients without toxicities (P < 0.0001 for all).
Conclusion: The newly developed chemotherapy regimens were associated with the decreased risk of mortality from CRC.
Keywords: cause-specific death; chemotherapy-related toxicity; colorectal cancer; comorbidity; newly developed chemotherapy regimens.
© The Author 2014. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Siegel R, DeSantis C, Jemal A. Colorectal cancer statistics, 2014. CA Cancer J Clin 2014; 64: 104–117. - PubMed
-
- Comparison of flourouracil with additional levamisole, higher-dose folinic acid, or both, as adjuvant chemotherapy for colorectal cancer: a randomised trial. QUASAR Collaborative Group. Lancet. 2000;355(9215):1588–1596. - PubMed
-
- Andre T, Boni C, Navarro M, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol. 2009;27(19):3109–3116. - PubMed
-
- Townsley CA, Selby R, Siu LL. Systematic review of barriers to the recruitment of older patients with cancer onto clinical trials. J Clin Oncol. 2005;23(13):3112–3124. - PubMed
-
- Aparicio T, Navazesh A, Boutron I, et al. Half of elderly patients routinely treated for colorectal cancer receive a sub-standard treatment. Crit Rev Oncol Hematol. 2009;71(3):249–257. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
