

Clinical comparison of distal pancreatectomy with or without splenectomy: a meta-analysis
- PMID: 24682038
- PMCID: PMC3969315
- DOI: 10.1371/journal.pone.0091593
Clinical comparison of distal pancreatectomy with or without splenectomy: a meta-analysis
Erratum in
- PLoS One. 2014;9(7):e103464
Abstract
Objective: A distal pancreatectomy has routinely been used for removing benign/borderline malignant tumors of the body and tail of the pancreas; however, controversy exists whether or not the spleen should be saved. Therefore, we conducted this meta-analysis for comparing the clinical outcomes of patients who underwent distal pancreatectomy with or without splenectomy.
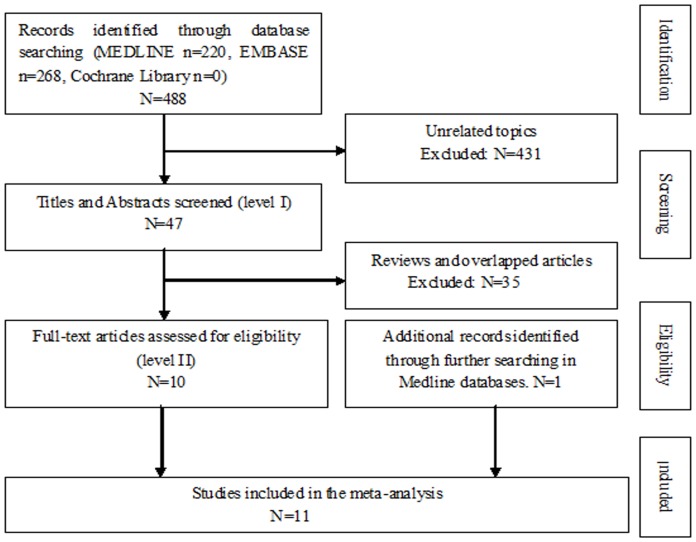
Methods: A literature research from the databases of Medline, Embase, and Cochrane library was performed to evaluate and compare the clinical outcomes between spleen-preserving distal pancreatectomy (SPDP) and distal pancreatectomy with splenectomy (DPS). Pooled odds ratio (OR) and weighted mean difference (WMD) with 95% confidence interval (95% CI) were calculated using fixed-effects or random-effects models.
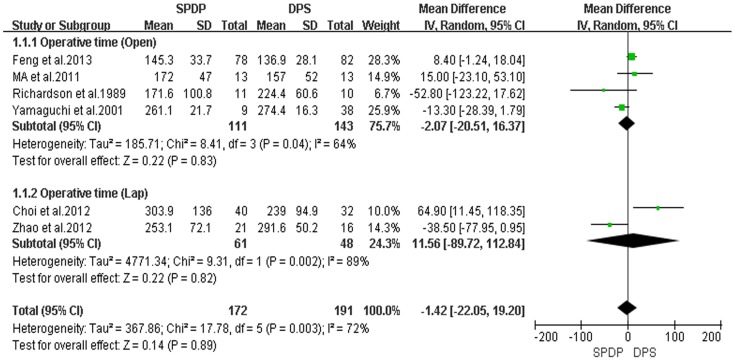
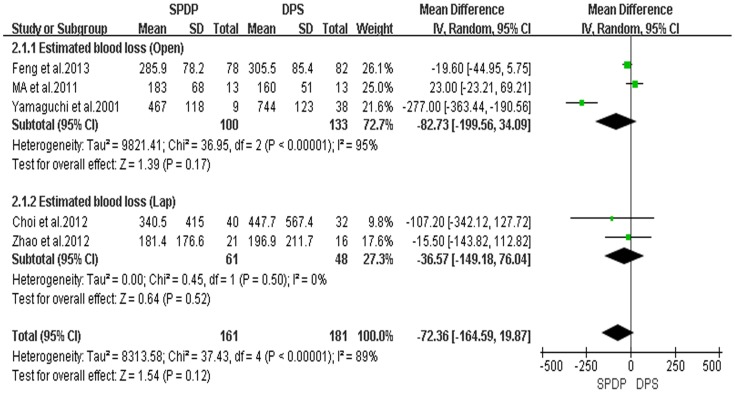
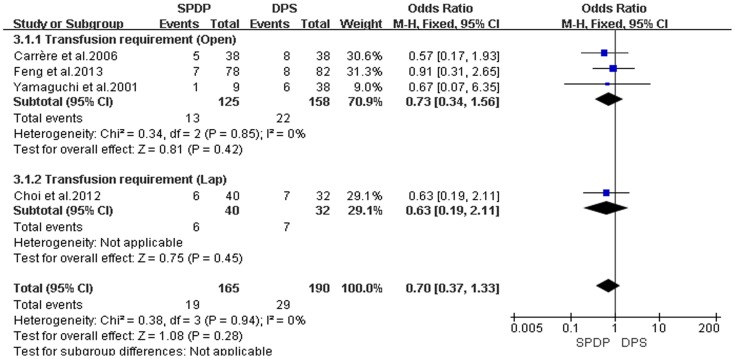
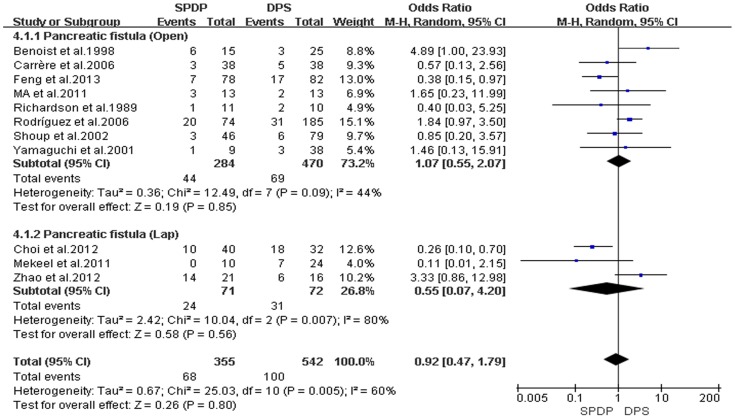
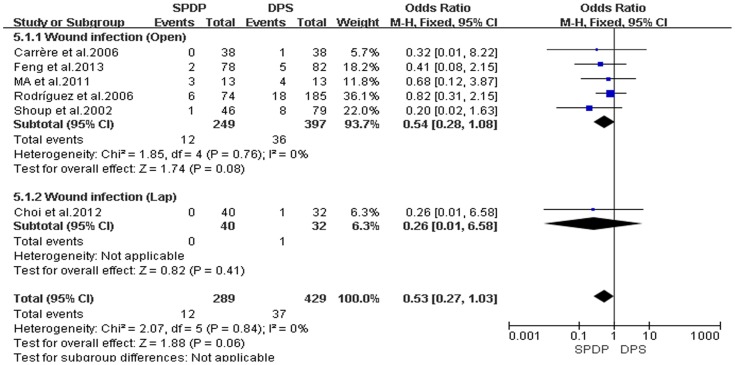
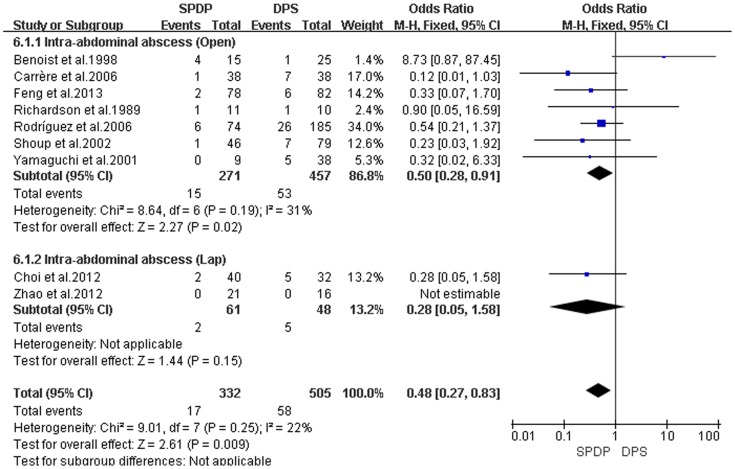
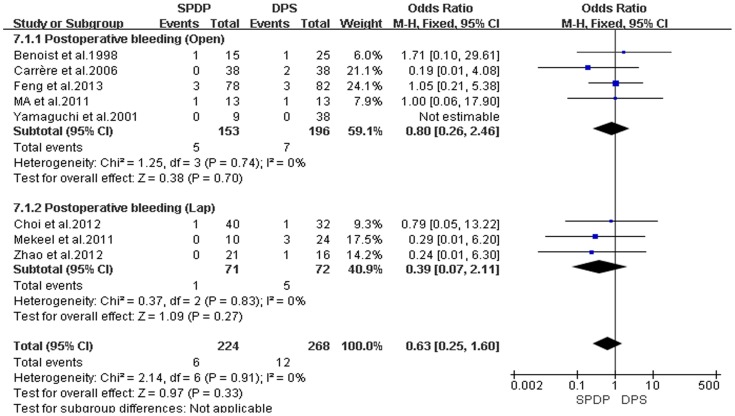
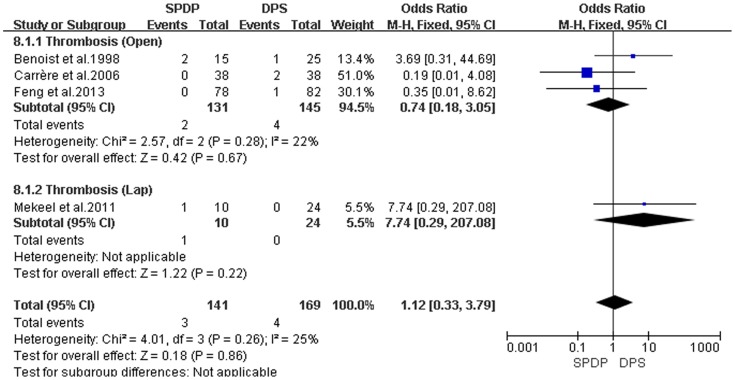
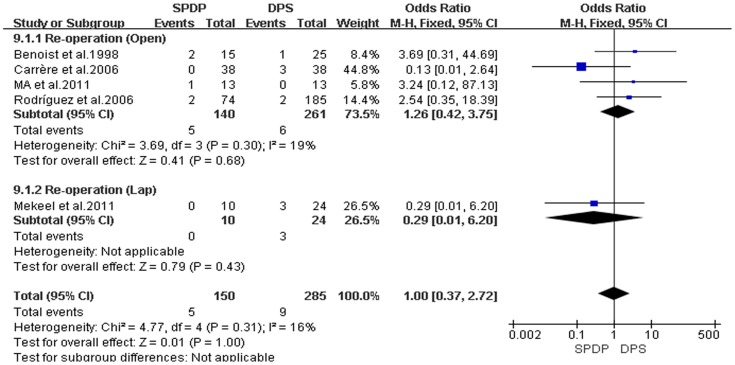
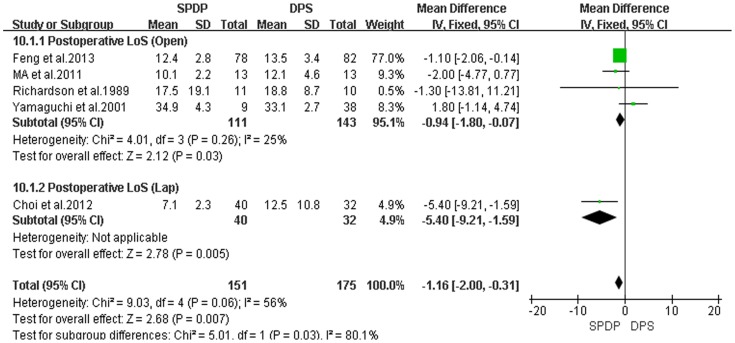
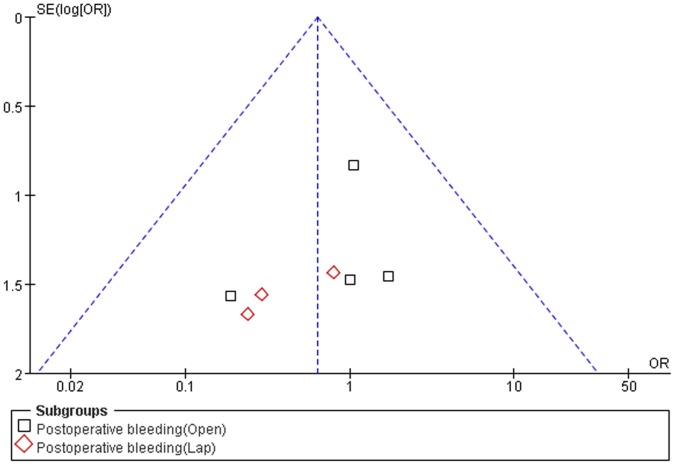
Results: Eleven non-randomized controlled studies involving 897 patients were selected to satisfy the inclusion criteria; 355 patients underwent SPDP and 542 patients underwent DPS. Compared with DPS, SPDP required a shorter hospital stay (WMD = 1.16, 95% CI = -2.00 to -0.31, P = 0.007), and had a lower incidence of intra-abdominal abscesses (OR = 0.48, 95% CI = 0.27 to 0.83, P = 0.009). In addition, spleen infarctions occurred in SPDP, most of which involved use of the Warshaw method for preserving the spleen. There were no differences between the SPDP and DPS groups with respect to operative time, operative blood loss, requirement for blood transfusion, pancreatic fistulas, thromboses, post-operative bleeding, wound infections and re-operation rates.
Conclusion: SPDP should be performed due to the benefits of the immune system and quick post-operative recovery. It is also essential to preserve the splenic artery and vein. Large randomized controlled trials are further needed to verify the results of this meta-analysis.
Conflict of interest statement
Figures
References
-
- Mellemkjaer L, Olsen JH, Linet MS, Gridley G, McLaughlin JK (1995) [Cancer risk after splenectomy]. Ugeskr Laeger 157: 5097–5100. - PubMed
-
- Bonenkamp J, Songun I, Welvaart K, van de Velde C, Hermans J, et al. (1995) Randomised comparison of morbidity after D1 and D2 dissection for gastric cancer in 996 Dutch patients. The Lancet 345: 745–748. - PubMed
-
- McGory ML, Zingmond DS, Sekeris E, Ko CY (2007) The significance of inadvertent splenectomy during colorectal cancer resection. Archives of Surgery 142: 668. - PubMed
-
- Espat NJ (2003) History of the Pancreas: Mysteries of a Hidden Organ. JAMA: The Journal of the American Medical Association 289: 1862–1863.
-
- Mallet-Guy P, Vachon A (1943) Pancreatites Chroniques Gauches: Paris.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
