

Lack of concordance between empirical scores and physician assessments of stroke and bleeding risk in atrial fibrillation: results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) registry
- PMID: 24682387
- PMCID: PMC4050636
- DOI: 10.1161/CIRCULATIONAHA.114.008643
Lack of concordance between empirical scores and physician assessments of stroke and bleeding risk in atrial fibrillation: results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) registry
Abstract
Background: Physicians treating patients with atrial fibrillation (AF) must weigh the benefits of anticoagulation in preventing stroke versus the risk of bleeding. Although empirical models have been developed to predict such risks, the degree to which these coincide with clinicians' estimates is unclear.
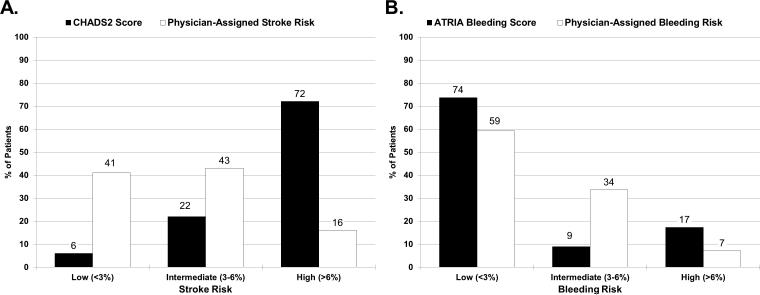
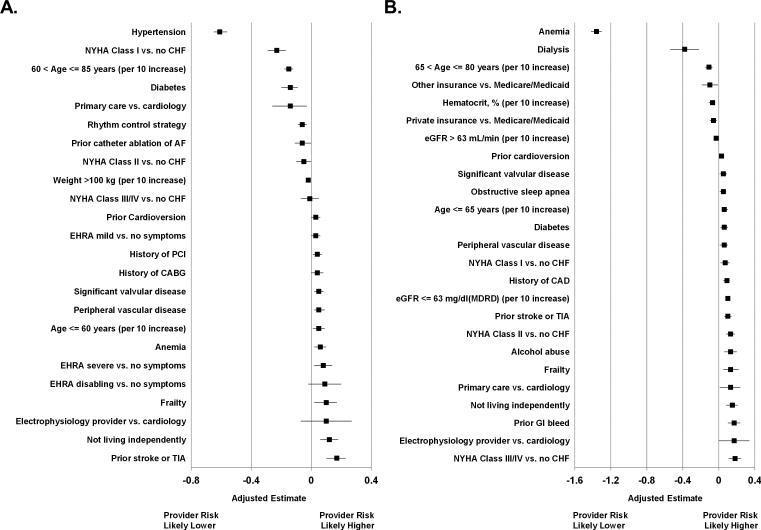
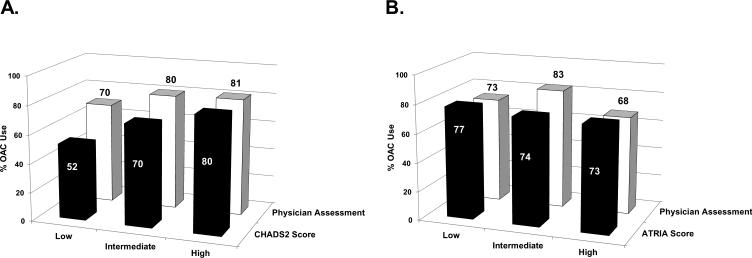
Methods and results: We examined 10 094 AF patients enrolled in the Outcomes Registry for Better Informed Treatment of AF (ORBIT-AF) registry between June 2010 and August 2011. Empirical stroke and bleeding risks were assessed by using the congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, and previous stroke or transient ischemic attack (CHADS2) and Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) scores, respectively. Separately, physicians were asked to categorize their patients' stroke and bleeding risks: low risk (<3%); intermediate risk (3%-6%); and high risk (>6%). Overall, 72% (n=7251) in ORBIT-AF had high-risk CHADS2 scores (≥2). However, only 16% were assessed as high stroke risk by physicians. Although 17% (n=1749) had high ATRIA bleeding risk (score ≥5), only 7% (n=719) were considered so by physicians. The associations between empirical and physician-estimated stroke and bleeding risks were low (weighted Kappa 0.1 and 0.11, respectively). Physicians weighed hypertension, heart failure, and diabetes mellitus less significantly than empirical models in estimating stroke risk; physicians weighted anemia and dialysis less significantly than empirical models when estimating bleeding risks. Anticoagulation use was highest among patients with high stroke risk, assessed by either empirical model or physician estimates. In contrast, physician and empirical estimates of bleeding had limited impact on treatment choice.
Conclusions: There is little agreement between provider-assessed risk and empirical scores in AF. These differences may explain, in part, the current divergence of anticoagulation treatment decisions from guideline recommendations.
Clinical trial registration url: http://www.clinicaltrials.gov. Unique identifier: NCT01165710.
Keywords: atrial fibrillation; hemorrhage; risk assessment; stroke.
© 2014 American Heart Association, Inc.
Figures
Comment in
-
Comparing the imperfect with the imperfect: the imprecise science of assessing the risk and benefits of anticoagulation in atrial fibrillation.Circulation. 2014 May 20;129(20):1997-9. doi: 10.1161/CIRCULATIONAHA.114.009979. Epub 2014 Mar 29. Circulation. 2014. PMID: 24682386 No abstract available.
-
Letter by Weinrauch and Barkoudah Regarding Article, "Lack of concordance between empirical scores and physician assessments of stroke and bleeding risk in atrial fibrillation. Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) Registry".Circulation. 2015 Feb 3;131(5):e335. doi: 10.1161/CIRCULATIONAHA.114.011869. Circulation. 2015. PMID: 25645616 No abstract available.
References
-
- Coyne KS, Paramore C, Grandy S, Mercader M, Reynolds M, Zimetbaum P. Assessing the direct costs of treating nonvalvular atrial fibrillation in the United States. Value Health. 2006;9:348–356. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983–988. - PubMed
-
- Ezekowitz MD, Levine JA. Preventing stroke in patients with atrial fibrillation. Jama. 1999;281:1830–1835. - PubMed
-
- Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. Jama. 2001;285:2864–2870. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
