

Dorsal root ganglionopathy is responsible for the sensory impairment in CANVAS
- PMID: 24682971
- PMCID: PMC4001192
- DOI: 10.1212/WNL.0000000000000352
Dorsal root ganglionopathy is responsible for the sensory impairment in CANVAS
Abstract
Objective: To elucidate the neuropathology in cerebellar ataxia with neuropathy and bilateral vestibular areflexia syndrome (CANVAS), a novel cerebellar ataxia comprised of the triad of cerebellar impairment, bilateral vestibular hypofunction, and a peripheral sensory deficit.
Method: Brain and spinal neuropathology in 2 patients with CANVAS, together with brain and otopathology in another patient with CANVAS, were examined postmortem.
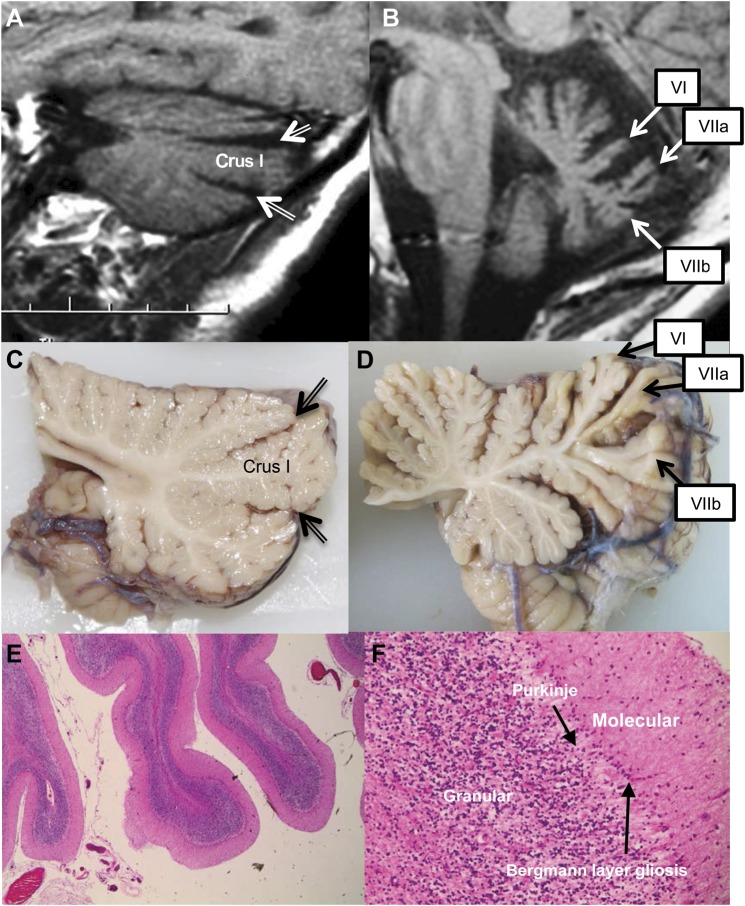
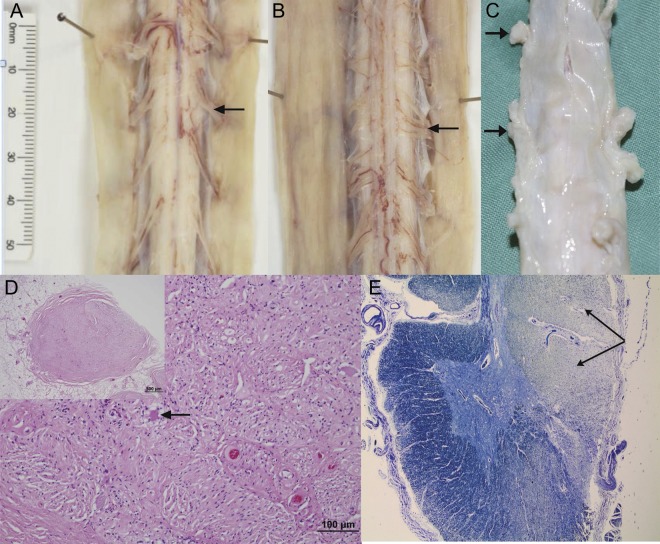
Results: Spinal cord pathology demonstrated a marked dorsal root ganglionopathy with secondary tract degeneration. Cerebellar pathology showed loss of Purkinje cells, predominantly in the vermis.
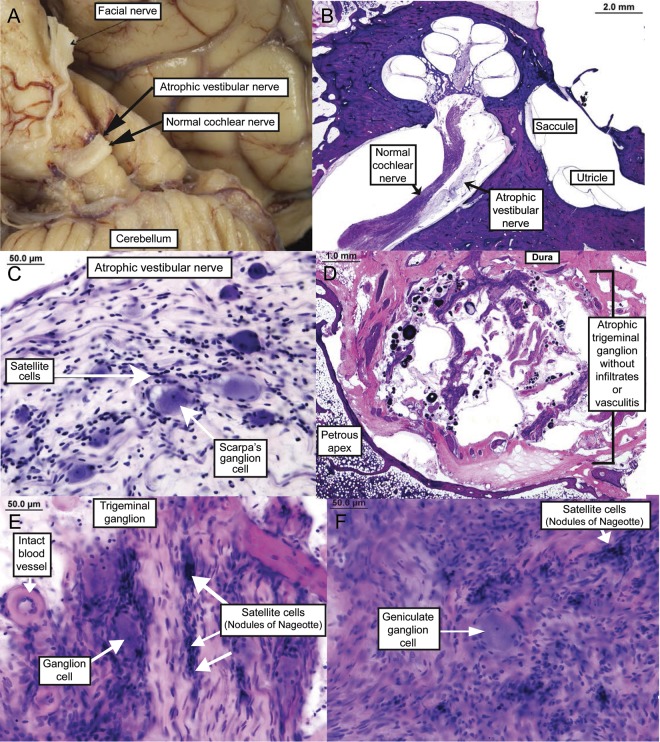
Conclusion: The likely underlying sensory pathology in CANVAS is loss of neurons from the dorsal root and V, VII, and VIII cranial nerve ganglia-in other words, it is a "neuronopathy" rather than a "neuropathy." Clinically, CANVAS is a differential diagnosis for both spinocerebellar ataxia type 3 (or Machado-Joseph disease) and Friedreich ataxia. In addition, there are 6 sets of sibling pairs, implying that CANVAS is likely to be a late-onset recessive or autosomal dominant with reduced penetrance disorder, and identification of the culprit gene is currently a target of investigation.
Figures
References
-
- Szmulewicz DJ, Waterston JA, MacDougall HG, et al. Cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS): a review of the clinical features and video-oculographic diagnosis. Ann NY Acad Sci 2011;1233:139–147 - PubMed
-
- Migliaccio A, Halmagyi G, Mcgarvie L, Cremer P. Cerebellar ataxia with bilateral vestibulopathy: description of a syndrome and its characteristic clinical sign. Brain 2004;127:280–293 - PubMed
-
- Koeppen AH, Morral JA, Davis AN, et al. The dorsal root ganglion in Friedreich's ataxia. Acta Neuropathol 2009;118:763–776 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources