

Noninvasive Diagnosis of NASH and Liver Fibrosis Within the Spectrum of NAFLD
- PMID: 24683373
- PMCID: PMC3969008
Noninvasive Diagnosis of NASH and Liver Fibrosis Within the Spectrum of NAFLD
Abstract
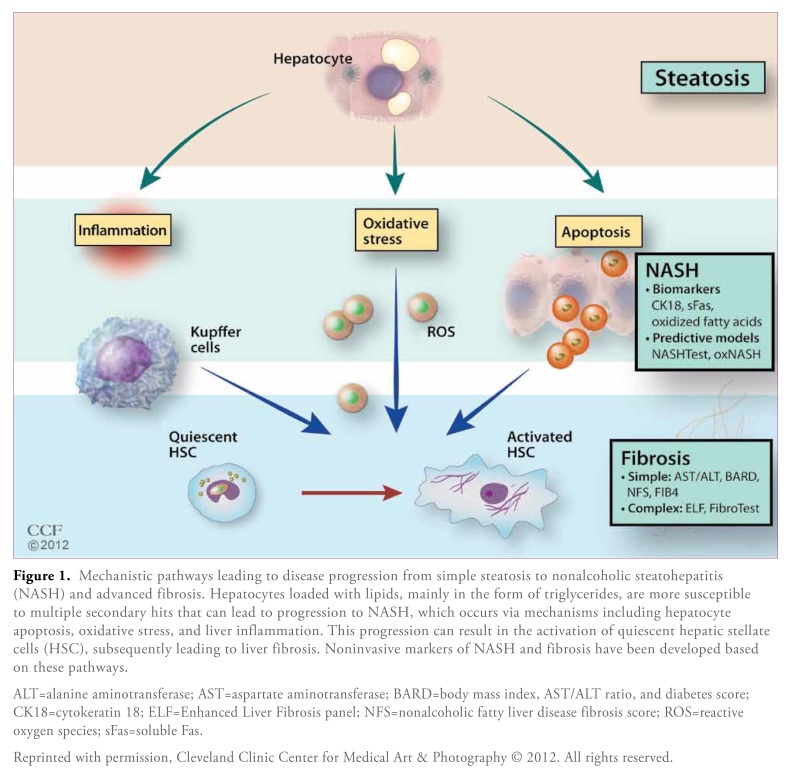
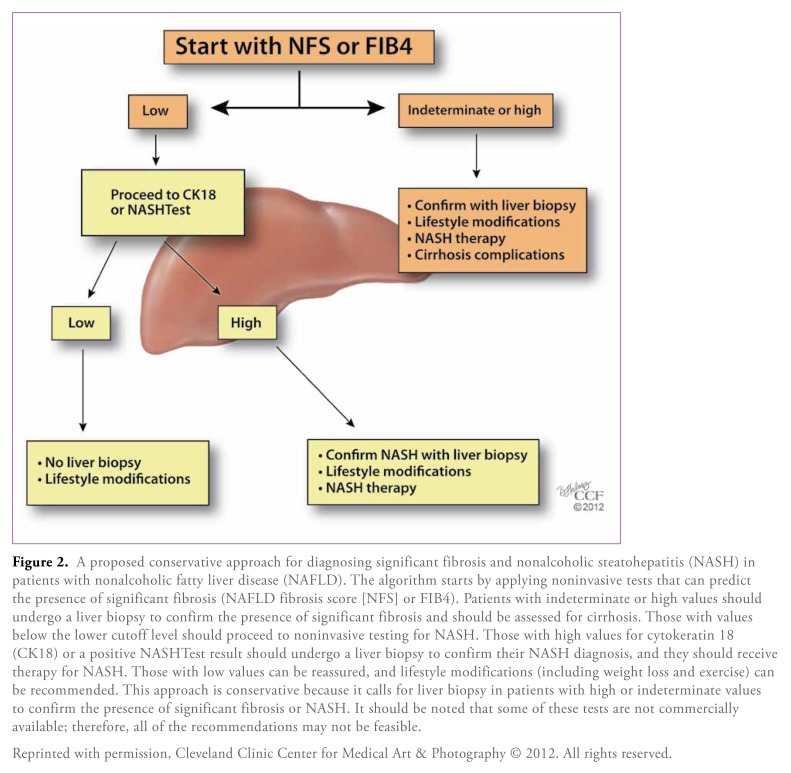
Nonalcoholic fatty liver disease (NAFLD) is the most common type of chronic liver disease in the United States, affecting an estimated 70 million Americans. The histologic spectrum of NAFLD ranges from simple steatosis to nonalcoholic steatohepatitis (NASH), fibrosis, and eventually cirrhosis. Patients with NASH and significant fibrosis seen on liver biopsy have an increased risk for liver-related morbidity and mortality compared to patients with simple steatosis. Due to the high prevalence of NAFLD, there has been an urgent need to develop reliable noninvasive markers and tests that can accurately predict the presence of advanced disease without the need for liver biopsy. These tests can be divided into 2 groups: those that predict the presence of NASH (such as markers of hepatocyte apoptosis, oxidative stress, and inflammation, as well as predictive models based on clinical variables) and those that predict the presence of fibrosis (such as simple and complex predictive models). This paper provides an overview of various noninvasive methods for detecting NAFLD and suggests a diagnostic algorithm that can be used in clinical practice.
Keywords: Nonalcoholic ratty liver disease; apoptosis; fibrosis; liver biopsy; nonalcoholic steatohepatitis; noninvasive markers; oxidative stress.
Figures
References
-
- Clark JM, Brancati FL, Diehl AM. Nonalcoholic fatty liver disease. Gastroenterology. 2002;122:1649–1657. - PubMed
-
- Wieckowska A, Feldstein AE. Nonalcoholic fatty liver disease in the pediatric population: a review. Curr Opin Pediatr. 2005;17:636–641. - PubMed
-
- Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002;346:1221–1231. - PubMed
-
- Browning JD, Szczepaniak LS, Dobbins R, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004;40:1387–1395. - PubMed
-
- Schwimmer JB, Deutsch R, Kahen T, Lavine JE, Stanley C, Behling C. Prevalence of fatty liver in children and adolescents. Pediatrics. 2006;118:1388–1393. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical