

doi: 10.1164/rccm.201312-2260LE.
Diaphragm fiber strength is reduced in critically ill patients and restored by a troponin activator
Affiliations
- PMID: 24684359
- PMCID: PMC4225832
- DOI: 10.1164/rccm.201312-2260LE
Item in Clipboard
Diaphragm fiber strength is reduced in critically ill patients and restored by a troponin activator
Am J Respir Crit Care Med.
.
No abstract available
Figures
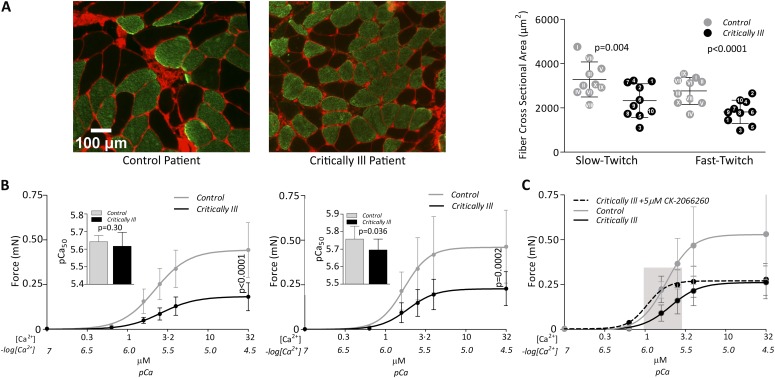
(A) Severe diaphragm muscle fiber atrophy in mechanically ventilated (MV) critically ill patients. Typical examples of serial diaphragm cross-sections stained with antibodies against slow-twitch myosin heavy chain (green). Wheat germ agglutinin (WGA) staining (red) was used to demarcate the muscle fibers. Scale bar = 100 μm (left panel). Quantification of, in total, 4,686 fibers revealed that, compared with control patients, fiber cross-sectional area (CSA) is 29% smaller in slow-twitch (control patients vs. critically ill patients: 3,284 ± 793 μm2 vs. 2,328 ± 763 μm2; P = 0.004) and 34% smaller in fast-twitch (control patients vs. intensive care unit [ICU] patients: 2,766 ± 606 μm2 vs. 1,819 ± 527 μm2; P < 0.0001) diaphragm muscle fibers of critically ill patients (right panel). Each dot with corresponding patient number indicates the mean CSA per patient (shaded dot, control patient; closed dot, critically ill patient). Horizontal bars indicate group mean; error bars indicate ±SD. (B) Severe diaphragm muscle fiber weakness in MV critically ill patients. Curves indicate the absolute force-calcium relation of diaphragm fibers of control patients and MV critically ill patients. Compared with control patients, the maximal absolute force—determined at maximally activating calcium concentrations (pCa 4.5)—was reduced by 56% in slow-twitch (control patients vs. ICU patients: 0.44 ± 0.16 mN vs. 0.19 ± 0.07 mN; P < 0.0001 [left panel]) and by 52% in fast-twitch (control patients vs. ICU patients: 0.49 ± 0.21 mN vs. 0.24 ± 0.09 mN; P = 0.0002 [right panel]) diaphragm fibers from critically ill patients. Indents show calcium sensitivity (pCa50). In slow-twitch fibers, pCa50 is not affected (control patients vs. critically ill patients: 5.64 ± 0.03 vs. 5.61 ± 0.08; P = 0.30 [left panel]), whereas in fast-twitch fibers pCa50 was significantly lower in critically ill patients (control patients vs. critically ill patients: 5.76 ± 0.07 vs. 5.70 ± 0.06; P = 0.036 [right panel]). Bullets and column bars indicate group mean; error bars indicate ±SD. (C) Diaphragm muscle fiber force is restored by a fast skeletal troponin activator. Curves show force response of fast-twitch fibers of a subset of patients to incremental calcium concentrations when exposed to vehicle (dimethyl sulfoxide [DMSO]) (gray solid line, control patients; black solid line, critically ill patients). Fibers from critically ill patients show a marked leftward shift of the force-calcium curve when treated with 5 μM CK-2066260 (dotted black line), such that, at physiological calcium concentration (indicated by gray bar), force is restored to levels observed in untreated fibers from control patients (force at pCa 5.8: 0.22 ± 0.05 mN [control patients with DMSO] vs. 0.22 ± 0.07 mN [critically ill patients with CK-2066260]; P = 0.954). Note that the magnitude of increase in pCa50 was comparable in both groups. Bullets indicate group mean; error bars indicate ±SD.
References
-
- Jaber S, Petrof BJ, Jung B, Chanques G, Berthet J-P, Rabuel C, Bouyabrine H, Courouble P, Koechlin-Ramonatxo C, Sebbane M, et al. Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans. Am J Respir Crit Care Med. 2011;183:364–371. - PubMed
-
- Watson AC, Hughes PD, Louise Harris M, Hart N, Ware RJ, Wendon J, Green M, Moxham J. Measurement of twitch transdiaphragmatic, esophageal, and endotracheal tube pressure with bilateral anterolateral magnetic phrenic nerve stimulation in patients in the intensive care unit. Crit Care Med. 2001;29:1325–1331. - PubMed
-
- Welvaart WN, Paul MA, Stienen GJ, van Hees HW, Loer SA, Bouwman R, Niessen H, de Man FS, Witt CC, Granzier H, et al. Selective diaphragm muscle weakness after contractile inactivity during thoracic surgery. Ann Surg. 2011;254:1044–1049. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
