

Renal transplantation using belatacept without maintenance steroids or calcineurin inhibitors
- PMID: 24684552
- PMCID: PMC4642731
- DOI: 10.1111/ajt.12712
Renal transplantation using belatacept without maintenance steroids or calcineurin inhibitors
Abstract
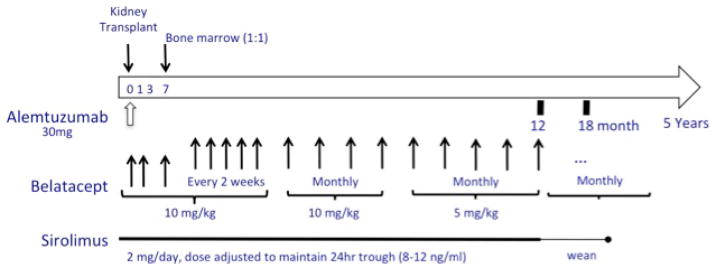
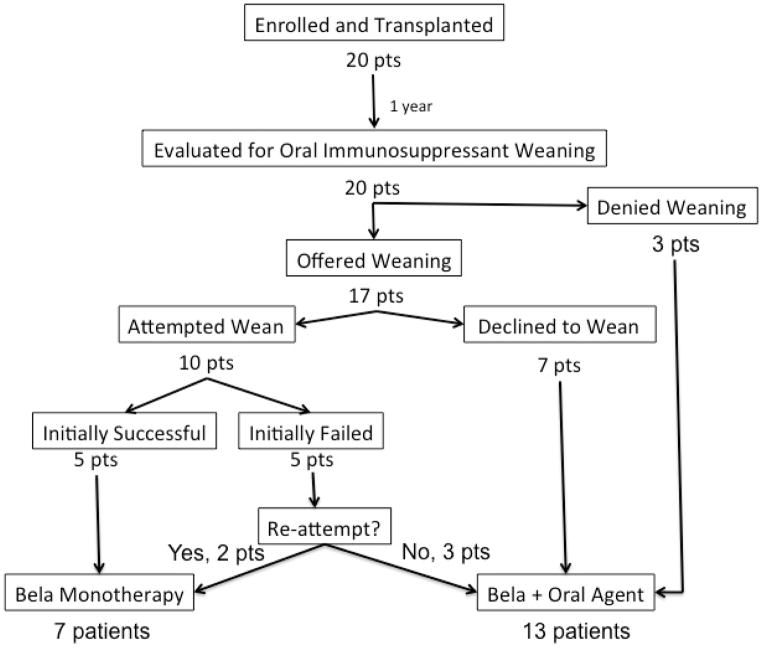
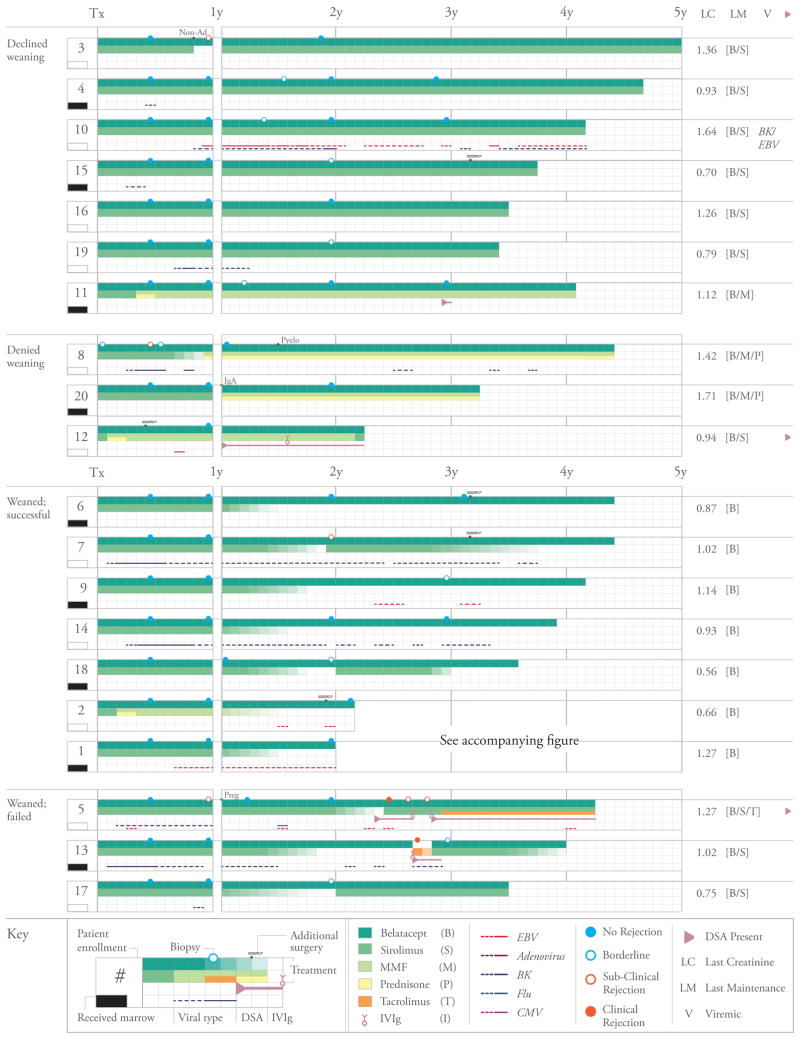
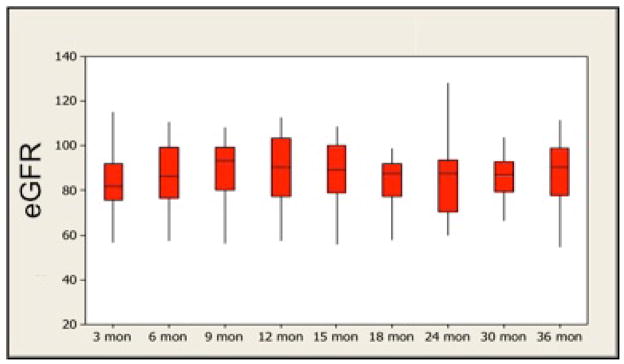
Kidney transplantation remains limited by toxicities of calcineurin inhibitors (CNIs) and steroids. Belatacept is a less toxic CNI alternative, but existing regimens rely on steroids and have higher rejection rates. Experimentally, donor bone marrow and sirolimus promote belatacept's efficacy. To investigate a belatacept-based regimen without CNIs or steroids, we transplanted recipients of live donor kidneys using alemtuzumab induction, monthly belatacept and daily sirolimus. Patients were randomized 1:1 to receive unfractionated donor bone marrow. After 1 year, patients were allowed to wean from sirolimus. Patients were followed clinically and with surveillance biopsies. Twenty patients were transplanted, all successfully. Mean creatinine (estimated GFR) was 1.10 ± 0.07 mg/dL (89 ± 3.56 mL/min) and 1.13 ± 0.07 mg/dL (and 88 ± 3.48 mL/min) at 12 and 36 months, respectively. Excellent results were achieved irrespective of bone marrow infusion. Ten patients elected oral immunosuppressant weaning, seven of whom were maintained rejection-free on monotherapy belatacept. Those failing to wean were successfully maintained on belatacept-based regimens supplemented by oral immunosuppression. Seven patients declined immunosuppressant weaning and three patients were denied weaning for associated medical conditions; all remained rejection-free. Belatacept and sirolimus effectively prevent kidney allograft rejection without CNIs or steroids when used following alemtuzumab induction. Selected, immunologically low-risk patients can be maintained solely on once monthly intravenous belatacept.
Trial registration: ClinicalTrials.gov NCT00565773.
Keywords: Alemtuzumab; belatacept; costimulation; immunosuppressive regimens; minimization/withdrawal; sirolimus.
© Copyright 2014 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures

Comment in
-
Re: Renal transplantation using belatacept without maintenance steroids or calcineurin inhibitors.J Urol. 2015 Mar;193(3):950. doi: 10.1016/j.juro.2014.11.026. Epub 2014 Nov 13. J Urol. 2015. PMID: 25765417 No abstract available.
References
-
- Organ Procurement and Transplantation Network (OPTN) and Scientific Registry or Transplant Recipients (SRTR) OPTN/SRTR 2010 Annual Data Report. Department of Health and Human Services, Health and Services Administration, Healthcare Systems Bureau, Division of Transplantation. Am J Transplant. 2012;12(Suppl1):S1–154.
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Transplant. 2009;9(Suppl 3):S1–155. - PubMed
-
- Lamb KE, Lodhi S, Meier-Kriesche HU. Long-term renal allograft survival in the United States: a critical reappraisal. Am J Transplant. 2011;11:450–462. - PubMed
-
- Larsen CP, Pearson TC, Adams AB, Tso P, Shirasugi N, Strobert E, Anderson D, Cowan S, Price K, Naemura J, Emswiler J, Greene J, Turk LA, Bajorath J, Townsend R, Hagerty D, Linsley PS, Peach RJ. Rational development of LEA29Y (belatacept), a high-affinity variant of CTLA4-Ig with potent immunosuppressive properties. Am J Transplant. 2005;5:443–453. - PubMed
-
- Vincenti F, Larsen C, Durrbach A, Wekerle T, Nashan B, Blancho G, Lang P, Grinyo J, Halloran PF, Solez K, Hagerty D, Levy E, Zhou W, Natarajan K, Charpentier B Belatacept Study Group. Costimulation blockade with belatacept in renal transplantation. N Engl J Med. 2005;353:770–781. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
