

Liver transplantation: immunosuppression and oncology
- PMID: 24685671
- PMCID: PMC4025587
- DOI: 10.1097/MOT.0000000000000069
Liver transplantation: immunosuppression and oncology
Abstract
Purpose of review: Long-term survival of liver transplant recipients is threatened by increased rates of de-novo malignancy and recurrence of hepatocellular carcinoma (HCC), both events tightly related to immunosuppression.
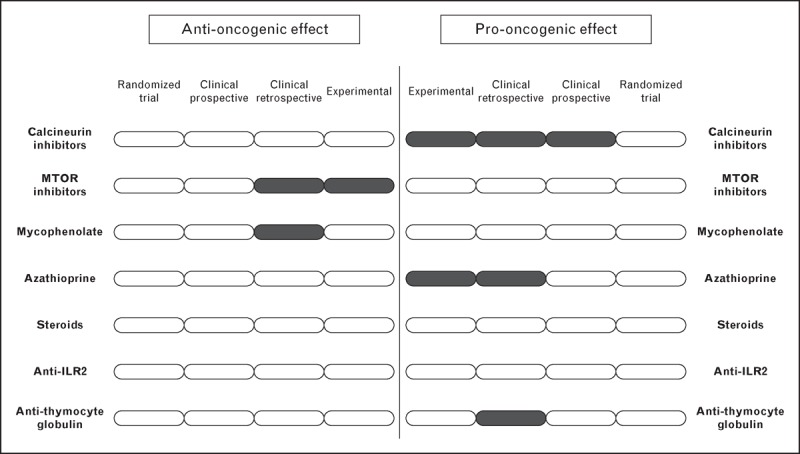
Recent findings: There is accumulating evidence linking increased exposure to immunosuppressants and carcinogenesis, particularly concerning calcineurin inhibitors (CNIs), azathioprine and antilymphocyte agents. A recent study including 219 HCC transplanted patients showed that HCC recurrence rates were halved if a minimization of CNIs was applied within the first month after liver transplant. With mammalian target of rapamycin (mTOR) inhibitors as approved immunosuppressants for liver transplant patients, pooled data from several retrospective studies have suggested their possible benefit for reducing HCC recurrence.
Summary: Randomized controlled trials with sufficiently long follow-up are needed to evaluate the influence of different immunosuppression protocols in preventing malignancy after LT. Currently, early minimization of CNIs with or without mTOR inhibitors or mycophenolate seems a rational strategy for patients with risk factors for de-novo malignancy or recurrence of HCC after liver transplant. A deeper understanding of the immunological pathways of rejection and cancer would allow for designing more specific and safer drugs, and thus to prevent cancer after liver transplant.
Figures
References
-
- Chandok N, Watt KD. Burden of de novo malignancy in the liver transplant recipient. Liver Transpl 2012; 18:1277–1289 - PubMed
-
This excellent review summarizes the impact of cancer on the prognosis after liver transplantation and highlights the most important risk factors.
-
- Aberg F, Pukkala E, Hockerstedt K, et al. Risk of malignant neoplasms after liver transplantation: a population-based study. Liver Transpl 2008; 14:1428–1436 - PubMed
-
- Baccarani U, Piselli P, Serraino D, et al. Comparison of de novo tumours after liver transplantation with incidence rates from Italian cancer registries. Dig Liver Dis 2010; 42:55–60 - PubMed
-
- Herrero JI, Lorenzo M, Quiroga J, et al. De Novo neoplasia after liver transplantation: an analysis of risk factors and influence on survival. Liver Transpl 2005; 11:89–97 - PubMed
-
- Jiang Y, Villeneuve PJ, Fenton SS, et al. Liver transplantation and subsequent risk of cancer: findings from a Canadian cohort study. Liver Transpl 2008; 14:1588–1597 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
