

Radiation enteropathy--pathogenesis, treatment and prevention
- PMID: 24686268
- PMCID: PMC4346191
- DOI: 10.1038/nrgastro.2014.46
Radiation enteropathy--pathogenesis, treatment and prevention
Abstract
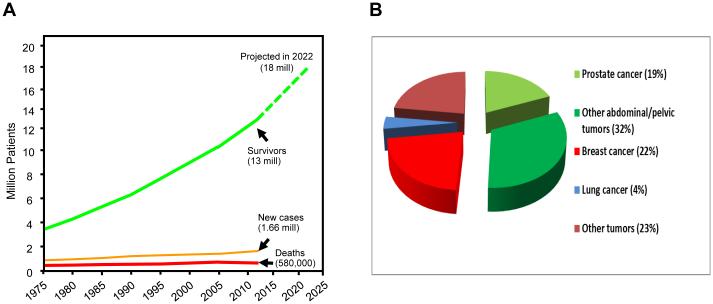
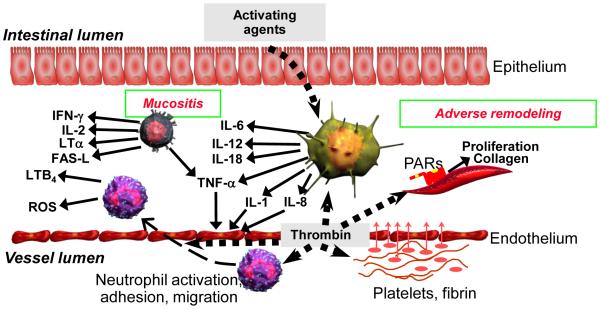
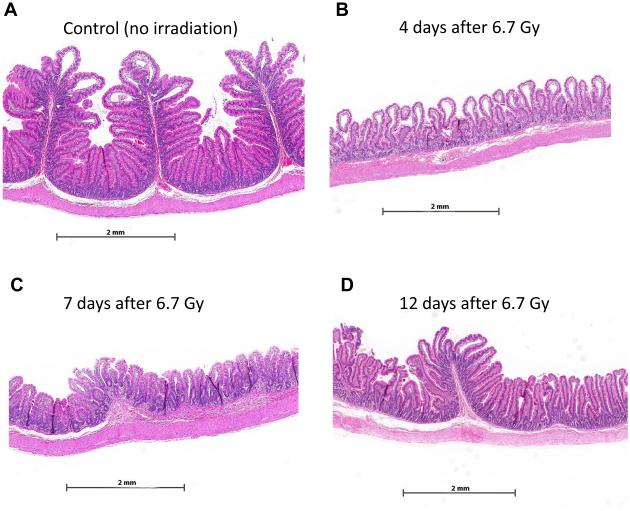
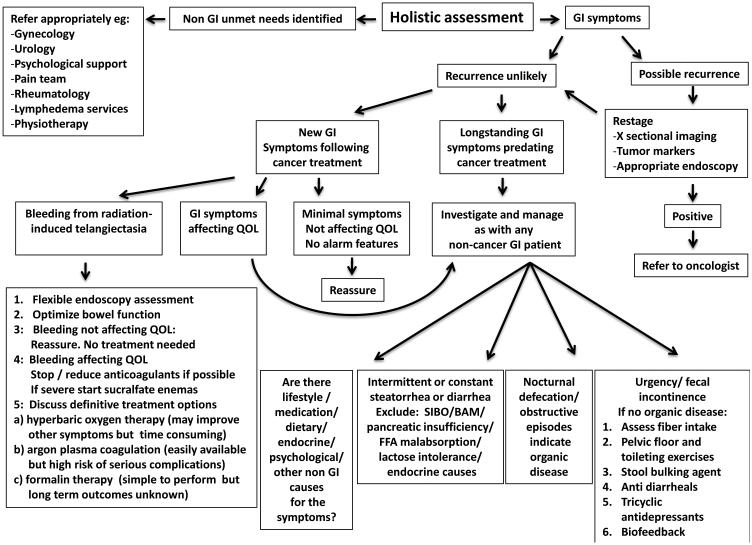
Changes in cancer incidence and mortality have been modest during the past several decades, but the number of cancer survivors has almost tripled during the same period. With an increasing cohort of cancer survivors, efforts to prevent, diagnose and manage adverse effects of cancer therapy, in general, and those of radiation therapy specifically, have intensified. Many cancer survivors have undergone radiation therapy of tumours in the pelvis or abdomen, thus rendering the bowel at risk of injury. In fact, the current prevalence of patients who have long-term radiation-induced intestinal adverse effects exceeds that of IBD. Considerable progress towards reducing toxicity of radiation therapy has been made by the introduction of so-called dose-sculpting treatment techniques, which enable precise delivery of the radiation beam. Moreover, new insights into the underlying pathophysiology have resulted in an improved understanding of mechanisms of radiation-induced bowel toxicity and in development of new diagnostic strategies and management opportunities. This Review discusses the pathogenesis of early and delayed radiation-induced bowel toxicity, presents current management options and outlines priorities for future research. By adding insight into molecular and cellular mechanisms of related bowel disorders, gastroenterologists can substantially strengthen these efforts.
Figures
References
-
- Goitein M. How best to dispose of extra-tumoral dose: a cautionary note for intensity-modulated radiation therapy. Int J Radiat Oncol Biol Phys. 2009;75:1–3. - PubMed
-
- Eifel PJ, Jhingran A, Bodurka DC, Levenback C, Thames H. Correlation of smoking history and other patient characteristics with major complications of pelvic radiation therapy for cervical cancer. J Clin Oncol. 2002;20:3651–3657. - PubMed
-
- Wedlake LJ, et al. Predicting late effects of pelvic radiotherapy: is there a better approach? Int J Radiat Oncol Biol Phys. 2010;78:1163–1170. - PubMed
-
- Willett CG, et al. Acute and late toxicity of patients with inflammatory bowel disease undergoing irradiation for abdominal and pelvic neoplasms. Int J Radiat Oncol Biol Phys. 2000;46:995–998. - PubMed
-
- Herold DM, Hanlon AL, Hanks GE. Diabetes mellitus: a predictor for late radiation morbidity. Int J Radiat Oncol Biol Phys. 1999;43:475–479. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
