

Associations between HIV infection and subclinical coronary atherosclerosis
- PMID: 24687069
- PMCID: PMC4143766
- DOI: 10.7326/M13-1754
Associations between HIV infection and subclinical coronary atherosclerosis
Abstract
Background: Coronary artery disease (CAD) has been associated with HIV infection, but data are not consistent.
Objective: To determine whether HIV-infected men have more coronary atherosclerosis than uninfected men.
Design: Cross-sectional study.
Setting: Multicenter AIDS Cohort Study.
Participants: HIV-infected (n = 618) and uninfected (n = 383) men who have sex with men who were aged 40 to 70 years, weighed less than 136 kg (200 lb), and had no history of coronary revascularization.
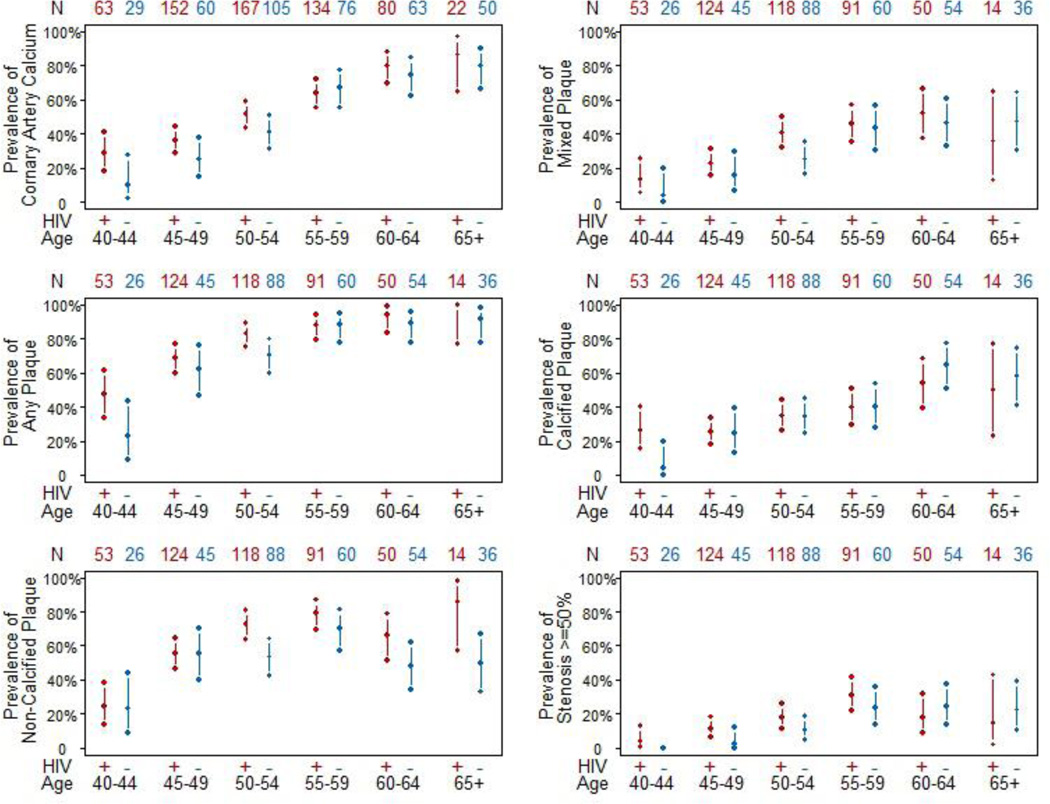
Measurements: Presence and extent of coronary artery calcium (CAC) on noncontrast cardiac computed tomography (CT) and of any plaque; noncalcified, mixed, or calcified plaque; or stenosis on coronary CT angiography.
Results: 1001 men had noncontrast CT, of whom 759 had coronary CT angiography. After adjustment for age, race, CT scanning center, and cohort, HIV-infected men had a greater prevalence of CAC (prevalence ratio [PR], 1.21 [95% CI, 1.08 to 1.35]; P = 0.001) and any plaque (PR, 1.14 [CI, 1.05 to 1.24]; P = 0.001), including noncalcified (PR, 1.28 [CI, 1.13 to 1.45]; P < 0.001) and mixed (PR, 1.35 [CI, 1.10 to 1.65]; P = 0.004) plaque, than uninfected men. Associations between HIV infection and any plaque or noncalcified plaque remained significant (P < 0.005) after CAD risk factor adjustment. HIV-infected men had a greater extent of noncalcified plaque after CAD risk factor adjustment (P = 0.026). They also had a greater prevalence of coronary artery stenosis greater than 50% (PR, 1.48 [CI, 1.06 to 2.07]; P = 0.020), but not after CAD risk factor adjustment. Longer duration of highly active antiretroviral therapy (PR, 1.09 [CI, 1.02 to 1.17]; P = 0.007) and lower nadir CD4+ T-cell count (PR, 0.80 [CI, 0.69 to 0.94]; P = 0.005) were associated with coronary stenosis greater than 50%.
Limitation: Cross-sectional observational study design and inclusion of only men.
Conclusion: Coronary artery plaque, especially noncalcified plaque, is more prevalent and extensive in HIV-infected men, independent of CAD risk factors.
Primary funding source: National Heart, Lung, and Blood Institute and National Institute of Allergy and Infectious Diseases.
Figures
Comment in
-
HIV infection and subclinical coronary atherosclerosis.Ann Intern Med. 2014 Dec 16;161(12):923. doi: 10.7326/L14-5033. Ann Intern Med. 2014. PMID: 25506860 No abstract available.
-
HIV infection and subclinical coronary atherosclerosis.Ann Intern Med. 2014 Dec 16;161(12):923-4. doi: 10.7326/L14-5033-2. Ann Intern Med. 2014. PMID: 25506861 No abstract available.
References
-
- May MT, Sterne JA, Costagliola D, et al. HIV treatment response and prognosis in Europe and North America in the first decade of highly active antiretroviral therapy: a collaborative analysis. Lancet. 2006;368:451. - PubMed
-
- Wada N, Jacobson LP, Cohen M, et al. Cause-specific life expectancies after 35 years of age for human immunodeficiency syndrome-infected and human immunodeficiency syndrome-negative individuals followed simultaneously in long-term cohort studies, 1984–2008. Am J Epidemiol. 2013;177(2):116–125. - PMC - PubMed
-
- Palella FJ, Jr, Baker RK, Moorman AC, Chmiel JS, Wood KC, Brooks JT, et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43(1):27–34. - PubMed
-
- Mary-Krause M, Cotte L, Simon A, et al. Increased risk of myocardial infarction with duration of protease inhibitor therapy in HIV-infected men. AIDS. 2003;17:2479. - PubMed
-
- Friis-Moller N, Reiss P, Sabin CA, et al. Class of antiretroviral drugs and the risk of myocardial infarction. N Engl J Med. 2007;356:1723. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous