

Primary thrombocytosis in children
- PMID: 24688110
- PMCID: PMC3971071
- DOI: 10.3324/haematol.2013.092684
Primary thrombocytosis in children
Abstract
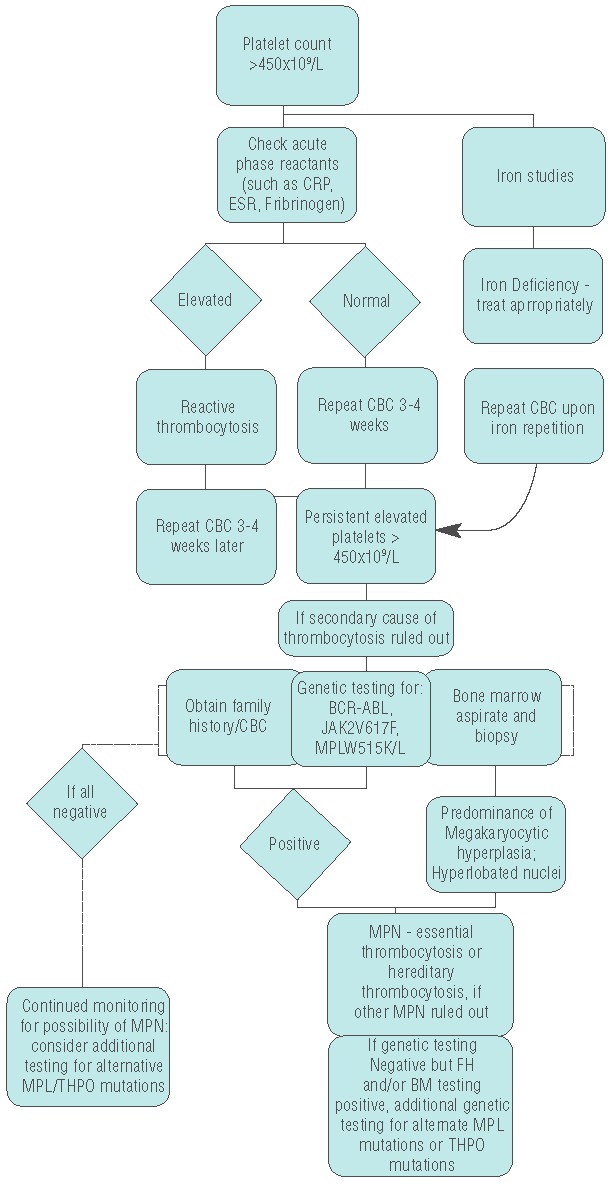
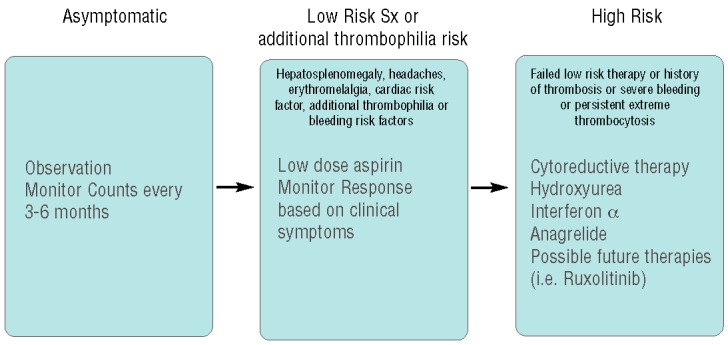
Myeloproliferative neoplasms are uncommon disorders in children, for which we have limited understanding of the pathogenesis and optimal management. JAK2 and MPL mutations, while common drivers of myeloproliferative neoplasms in adult patients, are not clearly linked to pediatric disease. Management and clinical outcomes in adults have been well delineated with defined recommendations for risk stratification and treatment. This is not the case for pediatric patients, for whom there is neither a standard approach to workup nor any consensus regarding management. This review will discuss thrombocytosis in children, including causes of thrombocytosis in children, the limited knowledge we have regarding pediatric primary thrombocytosis, and our thoughts on potential risk stratification and management, and future questions to be answered by laboratory research and collaborative clinical study.
Figures
Similar articles
-
Contemporary management of essential thrombocythemia in children.Expert Rev Hematol. 2019 May;12(5):367-373. doi: 10.1080/17474086.2019.1602034. Epub 2019 Apr 27. Expert Rev Hematol. 2019. PMID: 30925843 Review.
-
Thrombocytosis and thrombocythemia.Blood Rev. 2001 Dec;15(4):159-66. doi: 10.1054/blre.2001.0162. Blood Rev. 2001. PMID: 11792116 Review.
-
Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification and management.Am J Hematol. 2015 Feb;90(2):162-73. doi: 10.1002/ajh.23895. Am J Hematol. 2015. PMID: 25611051 Review.
-
Thrombocytosis in children and adolescents-classification, diagnostic approach, and clinical management.Ann Hematol. 2021 Jul;100(7):1647-1665. doi: 10.1007/s00277-021-04485-0. Epub 2021 Mar 12. Ann Hematol. 2021. PMID: 33712866 Free PMC article. Review.
-
[Diagnostic workup in front of an adult thrombocytosis].Ann Biol Clin (Paris). 2021 Oct 1;79(5):415-425. doi: 10.1684/abc.2021.1671. Ann Biol Clin (Paris). 2021. PMID: 34642137 French.
Cited by
-
Myeloproliferative Neoplasms in Children.J Hematop. 2015 Sep;8(3):143-157. doi: 10.1007/s12308-015-0256-1. Epub 2015 Aug 2. J Hematop. 2015. PMID: 26609329 Free PMC article.
-
Stuttering priapism in a pediatric patient with pheochromocytoma-induced thrombocytosis.Urol Ann. 2022 Jul-Sep;14(3):283-287. doi: 10.4103/ua.ua_118_21. Epub 2022 Jul 18. Urol Ann. 2022. PMID: 36117795 Free PMC article.
-
Extreme Thrombocytosis in a Child: Laboratory Approaches and Diagnostic Challenges.Oman Med J. 2019 Jul;34(4):336-340. doi: 10.5001/omj.2019.65. Oman Med J. 2019. PMID: 31360323 Free PMC article.
-
Myeloproliferative Neoplasms in Children, Adolescents, and Young Adults.Curr Hematol Malig Rep. 2020 Apr;15(2):141-148. doi: 10.1007/s11899-020-00571-8. Curr Hematol Malig Rep. 2020. PMID: 32172359 Free PMC article. Review.
-
Essential Thrombocythemia in Children and Adolescents.Cancers (Basel). 2021 Dec 6;13(23):6147. doi: 10.3390/cancers13236147. Cancers (Basel). 2021. PMID: 34885256 Free PMC article. Review.
References
-
- Dame C. Thrombocytosis. In: Arceci RJ, Hahn IM, Smith OP, eds. Pediatric Hematology. 3rd Ed. Oxford, UK: Blackwell Publishing Ltd; 2006, p.548–561
-
- Qian S, Fu F, Li W, Chen Q, de Sauvage FJ. Primary Role of the Liver in Thrombopoietin Production Shown by Tissue-Specific Knockout. Blood. 1998;92(6):2189–91 - PubMed
-
- Sungaran R, Markovic B, Chong BH. Localization and regulation of thrombopoietin mRNa expression in human kidney, liver, bone marrow, and spleen using in situ hybridization. Blood. 1997;89(1):101–7 - PubMed
-
- Kaushansky K, Lok S, Holly RD, Broudy VC, Lin N, Bailey MC, et al. Promotion of megakaryocyte progenitor expansion and differentiation by the c-Mpl ligand thrombopoietin. Nature. 1994;369(6481):568–71 - PubMed
-
- Zeigler FC, de Sauvage F, Widmer HR, Keller GA, Donahue C, Schreiber RD, et al. In vitro megakaryocytopoietic and thrombopoietic activity of c-mpl ligand (TPO) on purified murine hematopoietic stem cells. Blood. 1994;84(12):4045–52 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
