

Improving radiotherapy planning, delivery accuracy, and normal tissue sparing using cutting edge technologies
- PMID: 24688775
- PMCID: PMC3968554
- DOI: 10.3978/j.issn.2072-1439.2013.11.10
Improving radiotherapy planning, delivery accuracy, and normal tissue sparing using cutting edge technologies
Abstract
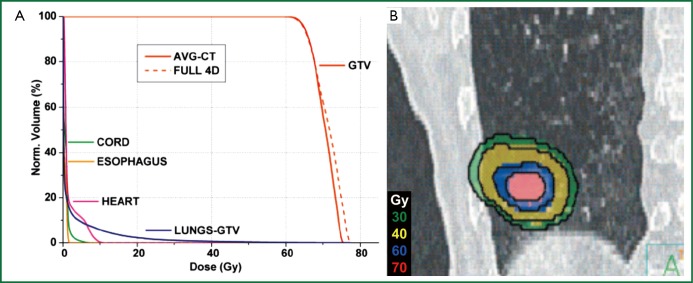
In the United States, more than half of all new invasive cancers diagnosed are non-small cell lung cancer, with a significant number of these cases presenting at locally advanced stages, resulting in about one-third of all cancer deaths. While the advent of stereotactic ablative radiation therapy (SABR, also known as stereotactic body radiotherapy, or SBRT) for early-staged patients has improved local tumor control to >90%, survival results for locally advanced stage lung cancer remain grim. Significant challenges exist in lung cancer radiation therapy including tumor motion, accurate dose calculation in low density media, limiting dose to nearby organs at risk, and changing anatomy over the treatment course. However, many recent technological advancements have been introduced that can meet these challenges, including four-dimensional computed tomography (4DCT) and volumetric cone-beam computed tomography (CBCT) to enable more accurate target definition and precise tumor localization during radiation, respectively. In addition, advances in dose calculation algorithms have allowed for more accurate dosimetry in heterogeneous media, and intensity modulated and arc delivery techniques can help spare organs at risk. New delivery approaches, such as tumor tracking and gating, offer additional potential for further reducing target margins. Image-guided adaptive radiation therapy (IGART) introduces the potential for individualized plan adaptation based on imaging feedback, including bulky residual disease, tumor progression, and physiological changes that occur during the treatment course. This review provides an overview of the current state of the art technology for lung cancer volume definition, treatment planning, localization, and treatment plan adaptation.
Keywords: Lung cancer; dose calculation; motion management; treatment planning.
Figures

References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin 2008;58:71-96 - PubMed
-
- Kong FM, Chetty IJ. Advancements in radiation therapy for medically inoperable early stage non-small cell lung cancer: leading article. Current Medical Literature, Respiratory Medicine 2006;20:57-65
-
- Hayman JA, Martel MK, Ten Haken RK, et al. Dose escalation in non-small-cell lung cancer using three-dimensional conformal radiation therapy: update of a phase I trial. J Clin Oncol 2001;19:127-36 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources