

The effectiveness and cost-effectiveness of lay counsellor-delivered psychological treatments for harmful and dependent drinking and moderate to severe depression in primary care in India: PREMIUM study protocol for randomized controlled trials
- PMID: 24690184
- PMCID: PMC4230277
- DOI: 10.1186/1745-6215-15-101
The effectiveness and cost-effectiveness of lay counsellor-delivered psychological treatments for harmful and dependent drinking and moderate to severe depression in primary care in India: PREMIUM study protocol for randomized controlled trials
Abstract
Background: The leading mental health causes of the global burden of disease are depression in women and alcohol use disorders in men. A major hurdle to the implementation of evidence-based psychological treatments in primary care in developing countries is the non-availability of skilled human resources. The aim of these trials is to evaluate the effectiveness and cost-effectiveness of two psychological treatments developed for the treatment of depression and alcohol use disorders in primary care in India.
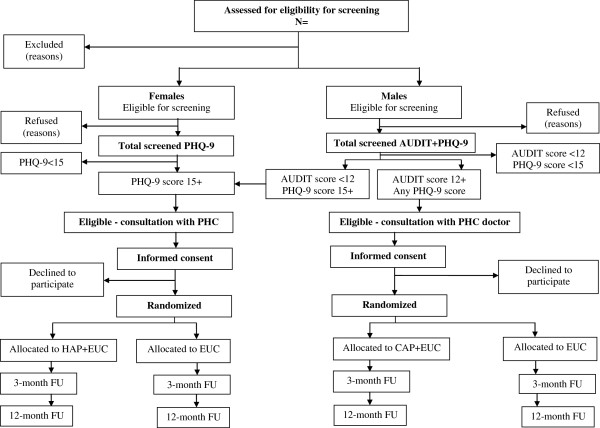
Methods/design: This study protocol is for parallel group, randomized controlled trials (Healthy Activity Program for moderate to severe depression, Counselling for Alcohol Problems for harmful and dependent drinking) in eight primary health centres in Goa, India. Adult primary care attendees will be screened with the Patient Health Questionnaire for depression and, in men only, the Alcohol Use Disorders Identification Test for drinking problems. Screen-positive attendees will be invited to participate; men who screen positive for both disorders will be invited to participate in the Counselling for Alcohol Problems trial. Those who consent will be allocated in a 1:1 ratio to receive either the respective psychological treatment plus enhanced usual care or enhanced usual care only using a computer generated allocation sequence, stratified by primary health centre and, for depression, by sex. The enhanced usual care comprises providing primary health centre doctors with contextualized World Health Organization guidelines and screening results. Psychological treatments will be delivered by lay counsellors, over a maximum period of three months. Primary outcomes are severity of disorder and remission rates at three months post-enrolment and, for the Counselling for Alcohol Problems trial, drinking and the impact of drinking on daily lives. Secondary outcomes include severity of disorder and remission rates at 12 months, disability scores, suicidal behaviour and economic impact, and cost-effectiveness at three and 12 months. 500 participants with depression and 400 participants with harmful drinking will be recruited. Primary analyses will be intention-to-treat.
Discussion: These trials may offer a new approach for the treatment of moderate-severe depression and drinking problems in primary care that is potentially scalable as it relies on delivery by a single pool of lay counsellors.
Trial registration: Both trials are registered with the International Society for the Registration of Clinical Trials (Healthy Activity Programme registration number ISRCTN95149997; Counselling for Alcohol Problems registration number ISRCTN76465238).
Figures
References
-
- Lopez AMC, Ezzati M, Jamison D, Murray C. Global Burden of Disease and Risk Factors. Washington: Oxford University Press and the World Bank; 2006.
-
- WHO. mhGAP Intervention Guide for Mental, Neurological and Substance Use Disorders in non-Specialized Health Settings. Geneva, Switzerland: WHO; 2010. - PubMed
-
- Wiles N, Thomas L, Abel A, Ridgway N, Turner N, Campbell J, Garland A, Hollinghurst S, Jerrom B, Kessler D, Kuyken W, Morrison J, Turner K, Williams C, Peters T, Lewis G. Cognitive behavioural therapy as an adjunct to pharmacotherapy for primary care based patients with treatment resistant depression: results of the CoBalT randomised controlled trial. Lancet. 2013;381:375–384. doi: 10.1016/S0140-6736(12)61552-9. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
