

Use of human fibrin glue (Tisseel) versus staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty (TISTA): a randomized controlled trial (NCT01641718)
- PMID: 24690207
- PMCID: PMC3994239
- DOI: 10.1186/1471-2482-14-18
Use of human fibrin glue (Tisseel) versus staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty (TISTA): a randomized controlled trial (NCT01641718)
Abstract
Background: Inguinal hernia repair is one of the most common surgical procedures worldwide. This procedure is increasingly performed with endoscopic techniques (laparoscopy). Many surgeons prefer to cover the hernia gap with a mesh to prevent recurrence. The mesh must be fixed tightly, but without tension. During laparoscopic surgery, the mesh is generally fixed with staples or tissue glue. However, staples often cause pain at the staple sites, and they can cause scarring of the abdominal wall, which can lead to chronic pain. We designed a trial that aims to determine whether mesh fixation with glue might cause less postoperative pain than fixation with staples during a transabdominal preperitoneal patch plastic repair.
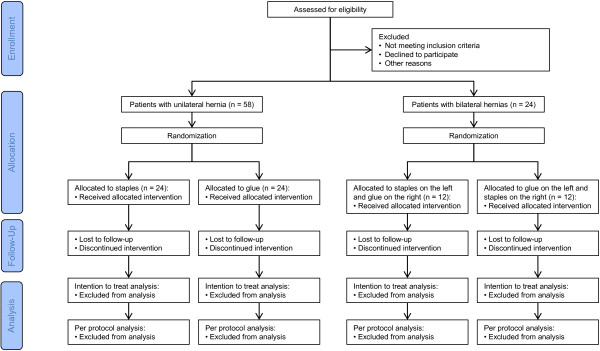
Methods/design: The TISTA trial is a prospective, randomized, controlled, single-center trial with a two-by-two parallel design. All patients and outcome-assessors will be blinded to treatment allocations. For eligibility, patients must be male, ≥18 years old, and scheduled for laparoscopic repair of a primary inguinal hernia. One group comprises patients with a unilateral inguinal hernia that will be randomized to receive mesh fixation with either tissue glue or staples. The second group comprises patients with bilateral inguinal hernias. They will be randomized to receive mesh fixation with tissue glue either on the right or the left side and with staples on the other side. The primary endpoint will be pain under physical stress, measured at 24 h after surgery. Pain will be rated by the patient based on a numeric rating scale from 0 to 10, where 10 equals the worst pain imaginable. A total of 82 patients will be recruited (58 patients with unilateral inguinal hernias and 24 patients with bilateral hernias). This number is estimated to provide 90% power for detecting a pain reduction of one point on a numeric rating scale, with a standard deviation of one.
Discussion: Patients with bilateral hernias will receive two meshes, one fixed with glue, and the other fixed with staples. This design will eliminate the inter-individual bias inherent in comparing pain measurements between two groups of patients.
Trial registration: ClinicalTrials.gov: NCT01641718.
Figures
Similar articles
-
Fibrin glue versus staple mesh fixation in single-port laparoscopic totally extraperitoneal inguinal hernia repair: A propensity score-matched analysis.Int J Surg. 2018 May;53:32-37. doi: 10.1016/j.ijsu.2018.01.029. Epub 2018 Feb 2. Int J Surg. 2018. PMID: 29410137
-
Staple versus fibrin glue fixation in laparoscopic total extraperitoneal repair of inguinal hernia: a systematic review and meta-analysis.Surg Endosc. 2012 May;26(5):1269-78. doi: 10.1007/s00464-011-2025-2. Epub 2012 Feb 21. Surg Endosc. 2012. PMID: 22350225
-
ARE THERE DIFFERENCES IN CHRONIC PAIN AFTER LAPAROSCOPIC INGUINAL HERNIA REPAIR USING THE TRANSABDOMINAL TECHNIQUE COMPARING WITH FIXATION OF THE MESH WITH STAPLES, WITH GLUE OR WITHOUT FIXATION? A CLINICAL RANDOMIZED, DOUBLE-BLIND TRIAL.Arq Bras Cir Dig. 2022 Sep 9;35:e1670. doi: 10.1590/0102-672020220002e1670. eCollection 2022. Arq Bras Cir Dig. 2022. PMID: 36102482 Free PMC article. Clinical Trial.
-
The impact of atraumatic fibrin sealant vs. staple mesh fixation in TAPP hernia repair on chronic pain and quality of life: results of a randomized controlled study.Surg Endosc. 2012 Jan;26(1):249-54. doi: 10.1007/s00464-011-1862-3. Epub 2011 Aug 19. Surg Endosc. 2012. PMID: 21853390 Clinical Trial.
-
Fibrin glue versus staple for mesh fixation in laparoscopic transabdominal preperitoneal repair of inguinal hernia: a meta-analysis and systematic review.Surg Endosc. 2017 Feb;31(2):527-537. doi: 10.1007/s00464-016-5039-y. Epub 2016 Jun 28. Surg Endosc. 2017. PMID: 27351657
Cited by
-
Current status and progress of laparoscopic inguinal hernia repair: A review.Medicine (Baltimore). 2023 Aug 4;102(31):e34554. doi: 10.1097/MD.0000000000034554. Medicine (Baltimore). 2023. PMID: 37543778 Free PMC article. Review.
References
-
- Suradom C, Palaphun J. The usage of two umbrella made-mesh plugs in herniorrhaphy: comparative study with Bassini and Lichtenstein method. J Med Assoc Thai. 2011;94:1373–1379. - PubMed
-
- Reuben B, Neumayer L. Surgical management of inguinal hernia. Adv Surg. 2006;40:299–317. - PubMed
-
- Camps J, Nguyen N, Annabali R, Fitzgibbons RJ Jr. Laparoscopic inguinal herniorrhaphy: transabdominal techniques. Int Surg. 1995;80:18–25. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
