

Did a quality improvement collaborative make stroke care better? A cluster randomized trial
- PMID: 24690267
- PMCID: PMC3997843
- DOI: 10.1186/1748-5908-9-40
Did a quality improvement collaborative make stroke care better? A cluster randomized trial
Abstract
Background: Stroke can result in death and long-term disability. Fast and high-quality care can reduce the impact of stroke, but UK national audit data has demonstrated variability in compliance with recommended processes of care. Though quality improvement collaboratives (QICs) are widely used, whether a QIC could improve reliability of stroke care was unknown.
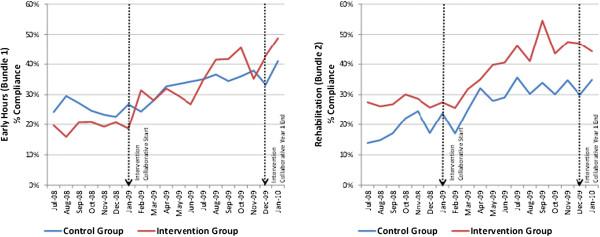
Methods: Twenty-four NHS hospitals in the Northwest of England were randomly allocated to participate either in Stroke 90:10, a QIC based on the Breakthrough Series (BTS) model, or to a control group giving normal care. The QIC focused on nine processes of quality care for stroke already used in the national stroke audit. The nine processes were grouped into two distinct care bundles: one relating to early hours care and one relating to rehabilitation following stroke. Using an interrupted time series design and difference-in-difference analysis, we aimed to determine whether hospitals participating in the QIC improved more than the control group on bundle compliance.
Results: Data were available from nine interventions (3,533 patients) and nine control hospitals (3,059 patients). Hospitals in the QIC showed a modest improvement from baseline in the odds of average compliance equivalent to a relative improvement of 10.9% (95% CI 1.3%, 20.6%) in the Early Hours Bundle and 11.2% (95% CI 1.4%, 21.5%) in the Rehabilitation Bundle. Secondary analysis suggested that some specific processes were more sensitive to an intervention effect.
Conclusions: Some aspects of stroke care improved during the QIC, but the effects of the QIC were modest and further improvement is needed. The extent to which a BTS QIC can improve quality of stroke care remains uncertain. Some aspects of care may respond better to collaboratives than others.
Trial registration: ISRCTN13893902.
Figures


References
-
- Institute for Healthcare Improvement. The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement (IHI Innovation Series white paper) Boston: Institute for Healthcare Improvement; 2003.
-
- Schouten LM, Hulscher ME, van Everdingen JJ, Huijsman R, Grol RP. Evidence for the impact of quality improvement collaboratives: systematic review. BMJ. 2008;336(7659):1491–1494. doi: 10.1136/bmj.39570.749884.BE. - DOI - PMC - PubMed
-
- Hulscher M, Schouten L, Grol R. Collaboratives. Nijmegen: Health Foundation; 2009.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
