

Patients with community acquired pneumonia admitted to European intensive care units: an epidemiological survey of the GenOSept cohort
- PMID: 24690444
- PMCID: PMC4056764
- DOI: 10.1186/cc13812
Patients with community acquired pneumonia admitted to European intensive care units: an epidemiological survey of the GenOSept cohort
Abstract
Introduction: Community acquired pneumonia (CAP) is the most common infectious reason for admission to the Intensive Care Unit (ICU). The GenOSept study was designed to determine genetic influences on sepsis outcome. Phenotypic data was recorded using a robust clinical database allowing a contemporary analysis of the clinical characteristics, microbiology, outcomes and independent risk factors in patients with severe CAP admitted to ICUs across Europe.
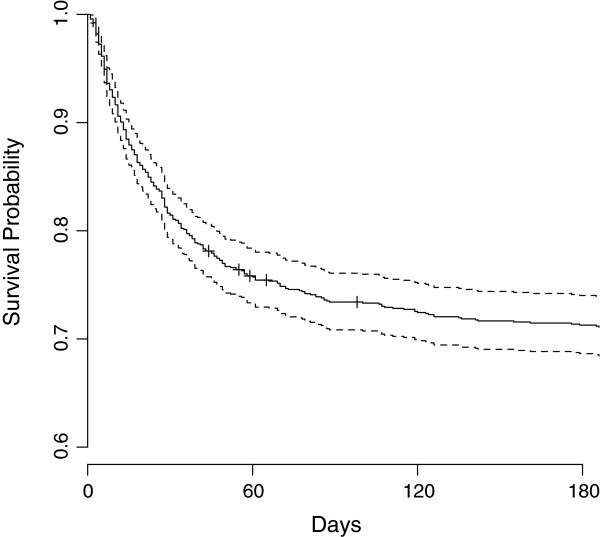
Methods: Kaplan-Meier analysis was used to determine mortality rates. A Cox Proportional Hazards (PH) model was used to identify variables independently associated with 28-day and six-month mortality.
Results: Data from 1166 patients admitted to 102 centres across 17 countries was extracted. Median age was 64 years, 62% were male. Mortality rate at 28 days was 17%, rising to 27% at six months. Streptococcus pneumoniae was the commonest organism isolated (28% of cases) with no organism identified in 36%. Independent risk factors associated with an increased risk of death at six months included APACHE II score (hazard ratio, HR, 1.03; confidence interval, CI, 1.01-1.05), bilateral pulmonary infiltrates (HR1.44; CI 1.11-1.87) and ventilator support (HR 3.04; CI 1.64-5.62). Haematocrit, pH and urine volume on day one were all associated with a worse outcome.
Conclusions: The mortality rate in patients with severe CAP admitted to European ICUs was 27% at six months. Streptococcus pneumoniae was the commonest organism isolated. In many cases the infecting organism was not identified. Ventilator support, the presence of diffuse pulmonary infiltrates, lower haematocrit, urine volume and pH on admission were independent predictors of a worse outcome.
Figures
References
-
- Woodhead MA, Macfarlane JT, McCracken JS, Rose DH, Finch RG. Prospective study of the aetiology and outcome of pneumonia in the community. Lancet. 1987;1:671–674. - PubMed
-
- Jokinen C, Heiskanen L, Juvonen H, Kallinen S, Karkola K, Korppi M, Kurki S, Ronnberg PR, Seppa A, Soimakallio S, Stén M, Tanska S, Tarkiainen A, Tukiainen H, Pyörälä K, Mäkelä PH. Incidence of community-acquired pneumonia in the population of four municipalities in eastern Finland. Am J Epidemiol. 1993;137:977–988. - PubMed
-
- Kellum JA, Kong L, Fink MP, Weissfeld LA, Yealy DM, Pinsky MR, Fine J, Krichevsky A, Delude RL, Angus DC. Understanding the inflammatory cytokine response in pneumonia and sepsis: results of the Genetic and Inflammatory Markers of Sepsis (GenIMS) Study. Arch Intern Med. 2007;167:1655–1663. doi: 10.1001/archinte.167.15.1655. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
