

Risk-scoring models for individualized prediction of overall survival in low-grade and high-grade endometrial cancer
- PMID: 24690476
- PMCID: PMC4405150
- DOI: 10.1016/j.ygyno.2014.03.567
Risk-scoring models for individualized prediction of overall survival in low-grade and high-grade endometrial cancer
Abstract
Objective: Overall survival (OS) in endometrial cancer (EC) is dependent on patient-, disease-, and treatment-specific risk factors. Comprehensive risk-scoring models were developed to estimate OS in low-grade and high-grade EC.
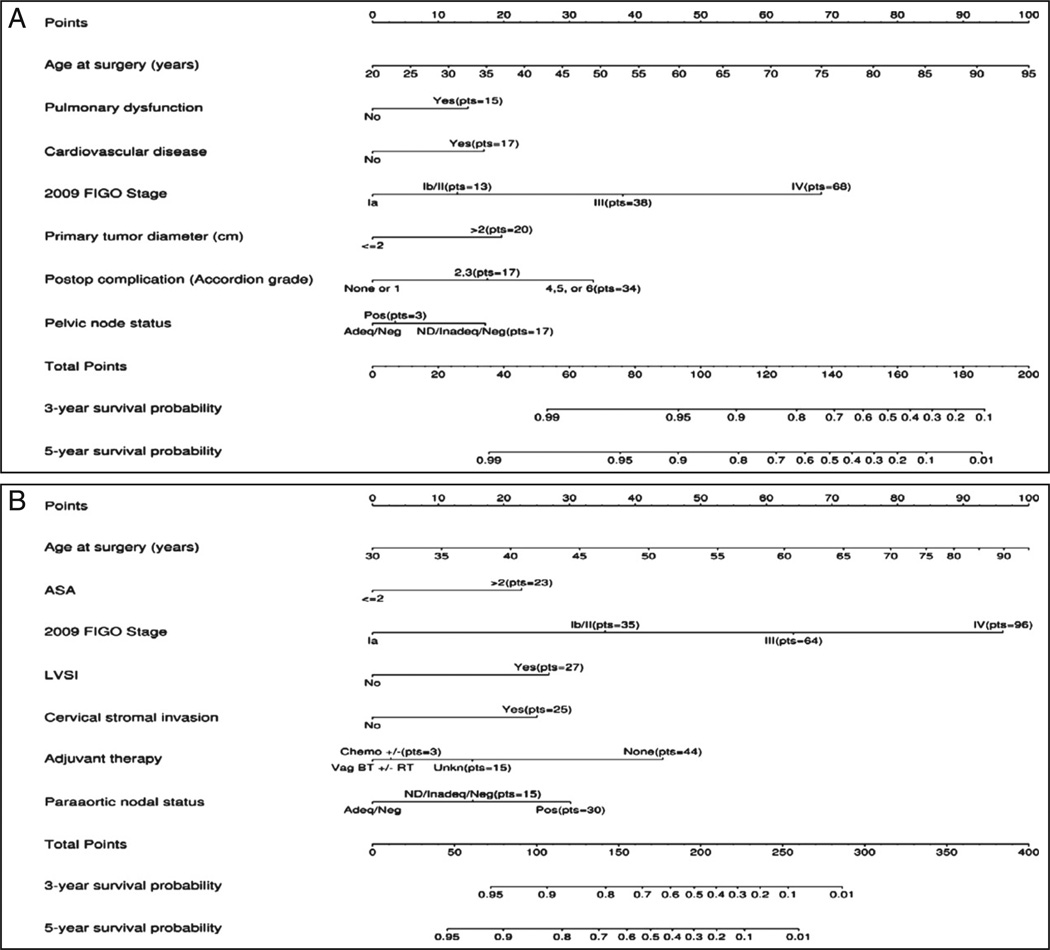
Methods: Patients undergoing primary surgery for EC from 1999 through 2008 were stratified histologically according to the International Federation of Gynecology and Obstetrics (FIGO) as either (i) low grade: grades 1 and 2 endometrioid EC or (ii) high grade: grade 3, including non-endometrioid EC. Associations between patient-, pathological-, and treatment-specific risk factors and OS starting on postoperative day 30 were assessed using multivariable Cox regression models. Factors independently associated with OS were used to construct nomograms and risk-scoring models.
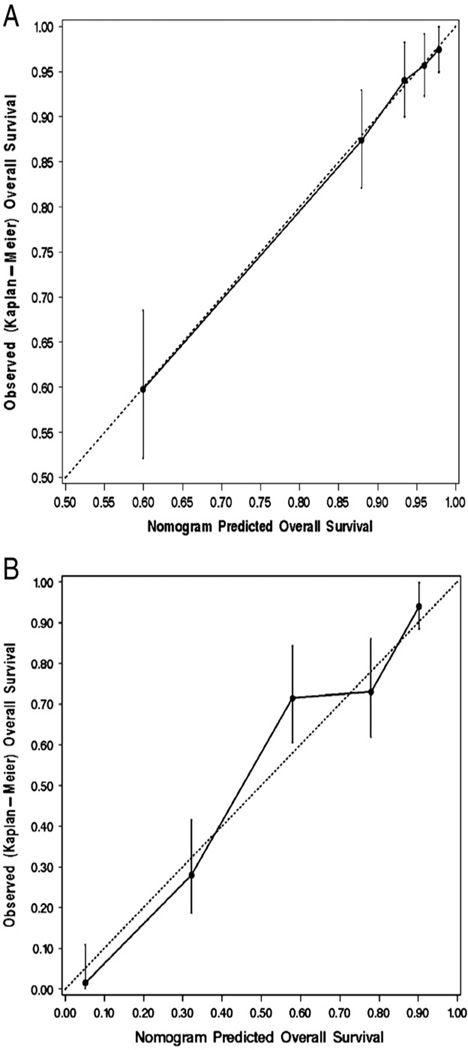
Results: Eligible patients (N=1281) included 925 low-grade and 356 high-grade patients; estimated 5-year OSs were 87.0% and 51.5%, respectively. Among patients alive at last follow-up, median follow-up was 5.0 (low grade) and 4.6years (high grade), respectively. In low-grade patients, independent factors predictive of compromised OS included age, cardiovascular disease, pulmonary dysfunction, stage, tumor diameter, pelvic lymph node status, and grade 2 or higher 30-day postoperative complications. Among high-grade patients, age, American Society of Anesthesiologists score, stage, lymphovascular space invasion, adjuvant therapy, para-aortic nodal status, and cervical stromal invasion were independent predictors of compromised OS. The two risk-scoring models/nomograms had excellent calibration and discrimination (unbiased c-indices=0.803 and 0.759).
Conclusion: Patients with low-grade and high-grade EC can be counseled regarding their predicted OS using the proposed risk-scoring models. This may facilitate institution of personalized treatment algorithms, surveillance strategies, and lifestyle interventions.
Keywords: Endometrial cancer; High grade; Low grade; Nomogram; Overall survival.
Copyright © 2014 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013 Jan;63(1):11–30. - PubMed
-
- Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol. 1983 Feb;15(1):10–17. - PubMed
-
- Creasman WT, Odicino F, Maisonneuve P, Quinn MA, Beller U, Benedet JL, et al. Carcinoma of the corpus uteri. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet. 2006 Nov;95(Suppl. 1):S105–S143. - PubMed
-
- Ward KK, Shah NR, Saenz CC, McHale MT, Alvarez EA, Plaxe SC. Cardiovascular disease is the leading cause of death among endometrial cancer patients. Gynecol Oncol. 2012 Aug;126(2):176–179. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
