

Review
doi: 10.1161/STROKEAHA.113.004534.
Epub 2014 Apr 1.
Multimodal markers of inflammation in the subcortical ischemic vascular disease type of vascular cognitive impairment
Affiliations
- PMID: 24692476
- PMCID: PMC4025998
- DOI: 10.1161/STROKEAHA.113.004534
Item in Clipboard
Review
Multimodal markers of inflammation in the subcortical ischemic vascular disease type of vascular cognitive impairment
Stroke.
2014 May.
No abstract available
Keywords: blood–brain barrier; cerebrospinal fluid; magnetic resonance imaging; matrix metalloproteinases.
Figures

Autopsy from a patient with Binswanger's disease that began at age 47 with death 7 years later. A) White matter gliosis was extensive as shown by GFAP staining. B) Arteriosclerotic changes in a arteriole in the white matter (H&E stain). C) Blood vessel is shown with thickening (PAS stain). D) Macrophages/microglia (CD68 immunostain) are seen around the arteriole in the white matter (Iba1 immunostain).

Schematic diagram of mechanism of white matter damage in SHR-SP. Hypoxia is postulated to be a key factor that triggers a series of molecular events. Generally there is hypertension, diabetes or other vasculopathic processes that restrict perfusion of the vulnerable deep white matter. Pyrol hydroxylase (PHD) is induced, leading to persistence of the HIF-1α. Multiple genes are activated, particularly MMP-2, which breaks down myelin and disrupts the blood-brain barrier (BBB). Vasogenic edema and oligodendrocytes death are the consequence of the hypoxia. Another pathway that includes the activation of inflammatory components induces MMP-3, MMP-9, and cyclooxygenase-2 (COX-2), contributing to the tissue damage. The entire process occurs slowly through the stages characterized as three “hits”: 1) Hypertension damages blood vessels, limiting blood flow to deep white matter; 2) Hypoxia initiates the molecular injury cascade as well as the repair mechanisms, such as angiogenesis and erythropoesis; and 3) An inflammatory response completes the injury process.
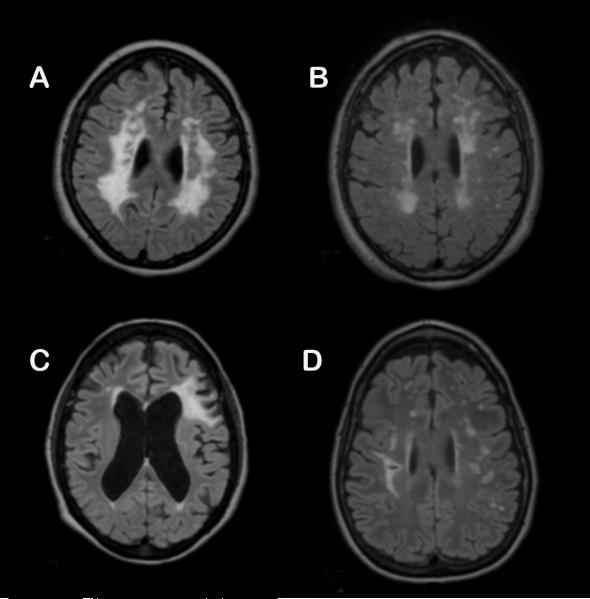
FLAIR MRI scans from representative patients in the different subgroups. A) Patient in the subcortical ischemic vascular disease (SIVD) group showing extensive white matter hyperintensities (WMHs) in a relatively symmetric distribution. B) Mixed VCI and AD (MX) patients have WMHs that are also symmetric. C) Multiple infarct (MI) patients have asymmetric lesions consistent with strokes. D) Leukoaraiosis (LA) patients have different patterns of WMHs that are difficult to characterize (permission received).

A) Square root WMH volume versus executive function T score (results are not significant with p=0.765), B) NAA and C) Cr versus executive function T score. Significance is p=0.056 for NAA and p<0.001 for Cr (permission received).

Permeability maps from three representative BD patients and two control patients. VCI1) A patient with large white matter hyperintensities (WMHs) on FLAIR (shown as the green areas). Arrows show increased permeability in subcortical and perilesion regions. Note the absence of permeability within the WMHs. VCI2 and VCI3 show additional patients. Controls show a small increase in permeability (red regions) in a nonspecific pattern. The regions of FLAIR increased signal were outlined with the semi-automated program (JIM) and colored green. The areas of increased permeability are seen as red and yellow (higher). There is very little increased permeability within the WMHs, but the increases occur around the lesions. (Courtesy of Arvind Caprihan, MIND Research Network, Albuquerque, NM).
References
-
- Bowler JV. Modern concept of vascular cognitive impairment. Br Med Bull. 2007;83:291–305. - PubMed
-
- Gold G, Giannakopoulos P, Herrmann FR, Bouras C, Kovari E. Identification of alzheimer and vascular lesion thresholds for mixed dementia. Brain. 2007;130:2830–2836. - PubMed
-
- Schneider JA, Arvanitakis Z, Bang W, Bennett DA. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology. 2007;69:2197–2204. - PubMed
-
- De Reuck J, Crevits L, De Coster W, Sieben G, vander Eecken H. Pathogenesis of binswanger chronic progressive subcortical encephalopathy. Neurology. 1980;30:920–928. - PubMed
-
- Olszewski J. Subcortical arteriosclerotic encephalopathy: Review of the literature on the so-called binswanger's disease and presentation of 2 cases. World Neurology. 1962;3:359–375. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
