

CTO pathophysiology: how does this affect management?
- PMID: 24694103
- PMCID: PMC4021289
- DOI: 10.2174/1573403x10666140331142349
CTO pathophysiology: how does this affect management?
Abstract
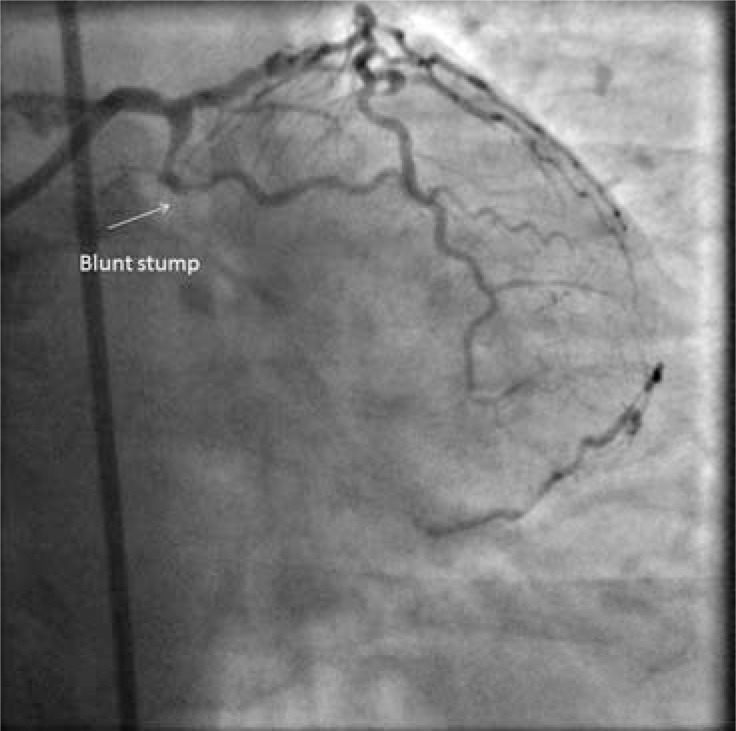
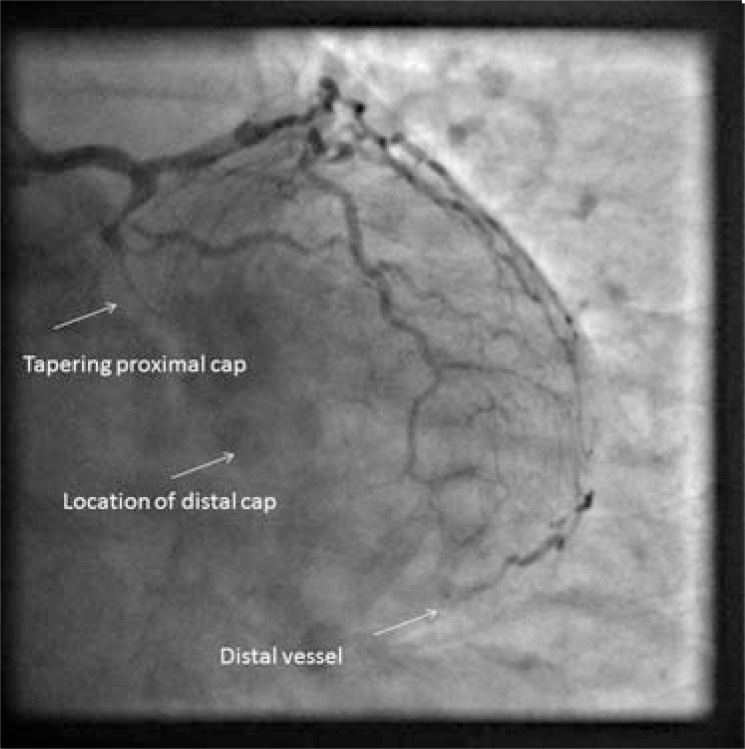
Chronic total occlusion (CTO) pathophysiology has been described in a few, small studies using post mortem histology, and more recently, in vivo intravascular ultrasound (IVUS) to analyse the constituents of occluded segments. Recent improvements in equipment and techniques have revealed new insights into physical characteristics of occluded coronaries, which in turn enable predictable procedural success. The purpose of this review is to consider the published evidence describing CTO pathophysiology from the perspective of the hybrid algorithm approach to CTO PCI.
Methods: Literature searches using "Chronic Occlusion", "angioplasty", and" pathology" as keywords. Further searches on "coronary" "collateral", "Viability". Bibliographies were scrutinised for further key publications in an iterative process. Papers describing animal models were excluded.
Figures



Similar articles
-
Initial success rate of percutaneous coronary intervention for chronic total occlusion in a native coronary artery is decreased in patients who underwent previous coronary artery bypass graft surgery.JACC Cardiovasc Interv. 2014 Jan;7(1):39-46. doi: 10.1016/j.jcin.2013.08.012. JACC Cardiovasc Interv. 2014. PMID: 24456717
-
Validation and incremental value of the hybrid algorithm for CTO PCI.Catheter Cardiovasc Interv. 2014 Oct 1;84(4):654-9. doi: 10.1002/ccd.25370. Epub 2014 Feb 4. Catheter Cardiovasc Interv. 2014. PMID: 24403122
-
Intravascular ultrasound guidance of percutaneous coronary intervention in ostial chronic total occlusions: a description of the technique and procedural results.Int J Cardiovasc Imaging. 2017 Jun;33(6):807-813. doi: 10.1007/s10554-017-1086-2. Epub 2017 Feb 14. Int J Cardiovasc Imaging. 2017. PMID: 28197870
-
Algorithmic solutions to common problems encountered during chronic total occlusion angioplasty: The algorithms within the algorithm.Catheter Cardiovasc Interv. 2019 Feb 1;93(2):286-297. doi: 10.1002/ccd.27987. Epub 2018 Nov 23. Catheter Cardiovasc Interv. 2019. PMID: 30467958 Review.
-
Update on the Management of Chronic Total Occlusions in Coronary Artery Disease.Curr Atheroscler Rep. 2017 Apr;19(4):19. doi: 10.1007/s11883-017-0655-0. Curr Atheroscler Rep. 2017. PMID: 28315181 Review.
Cited by
-
Coronary chronic total occlusion intervention: A pathophysiological perspective.Indian Heart J. 2018 Jul-Aug;70(4):548-555. doi: 10.1016/j.ihj.2018.01.021. Epub 2018 Jan 10. Indian Heart J. 2018. PMID: 30170652 Free PMC article. Review.
-
Impact of impaired renal function on outcomes of chronic total occlusion undergoing revascularization: a systemic review and meta-analysis.Int Urol Nephrol. 2022 Dec;54(12):3179-3191. doi: 10.1007/s11255-022-03192-7. Epub 2022 Jun 11. Int Urol Nephrol. 2022. PMID: 35689780
-
Delayed spontaneous recanalization of chronic total occlusion of left anterior descending artery after attempted but failed revascularization during percutaneous coronary intervention.J Community Hosp Intern Med Perspect. 2018 Aug 23;8(4):223-226. doi: 10.1080/20009666.2018.1490140. eCollection 2018. J Community Hosp Intern Med Perspect. 2018. PMID: 30181831 Free PMC article.
-
A Novel Classification for Predicting Chronic Total Occlusion Percutaneous Coronary Intervention.Front Cardiovasc Med. 2022 Feb 28;9:762351. doi: 10.3389/fcvm.2022.762351. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35295265 Free PMC article.
-
Retrograde Approach to Manage Acute Coronary Closure Due to Dissection.JACC Case Rep. 2025 May 21;30(11):103326. doi: 10.1016/j.jaccas.2025.103326. Epub 2025 Apr 9. JACC Case Rep. 2025. PMID: 40409862 Free PMC article.
References
-
- Christofferson RD, Lehmann KG, Martin GV, Every N, Caldwell JH, Kapadia SR. Effect of chronic total coronary occlusion on treatment strategy. The Am J Cardiol. 2005;95(9):1088–91. - PubMed
-
- Werner GS, Gitt AK, Zeymer U , et al. Chronic total coronary occlusions in patients with stable angina pectoris: impact on therapy and outcome in present day clinical practice. Clin Res Cardiol. 2009;98(7):435–41. - PubMed
-
- Fefer P, Knudtson ML, Cheema AN , et al. Current Perspectives on Coronary Chronic Total OcclusionsThe Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol. 2012;59(11):991–7. - PubMed
-
- Levin D. Pathways and functional significance of the coronary collateral circulation. Circulation. 1974;50(4):831–7. - PubMed
-
- Tubbs RS, Loukas M, Shoja MM, Ardalan MR, Oakes WJ. Richard Lower (1631-1691) and his early contributions to cardiology. Int J Cardiol. 2008;128(1):17–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
