

Image quality in thoracic 4D cone-beam CT: a sensitivity analysis of respiratory signal, binning method, reconstruction algorithm, and projection angular spacing
- PMID: 24694143
- PMCID: PMC3978414
- DOI: 10.1118/1.4868510
Image quality in thoracic 4D cone-beam CT: a sensitivity analysis of respiratory signal, binning method, reconstruction algorithm, and projection angular spacing
Abstract
Purpose: Respiratory signal, binning method, and reconstruction algorithm are three major controllable factors affecting image quality in thoracic 4D cone-beam CT (4D-CBCT), which is widely used in image guided radiotherapy (IGRT). Previous studies have investigated each of these factors individually, but no integrated sensitivity analysis has been performed. In addition, projection angular spacing is also a key factor in reconstruction, but how it affects image quality is not obvious. An investigation of the impacts of these four factors on image quality can help determine the most effective strategy in improving 4D-CBCT for IGRT.
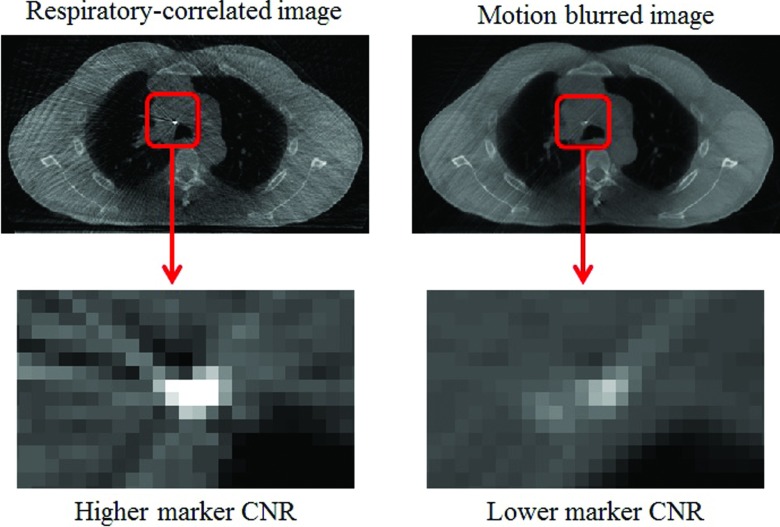
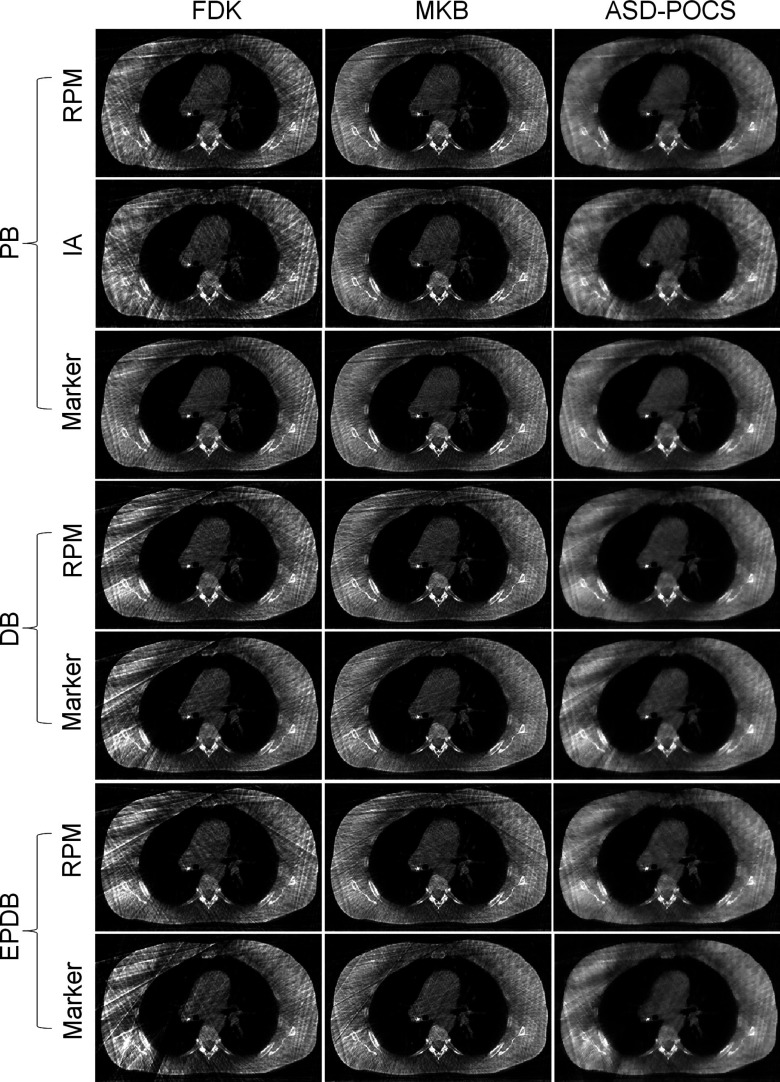
Methods: Fourteen 4D-CBCT patient projection datasets with various respiratory motion features were reconstructed with the following controllable factors: (i) respiratory signal (real-time position management, projection image intensity analysis, or fiducial marker tracking), (ii) binning method (phase, displacement, or equal-projection-density displacement binning), and (iii) reconstruction algorithm [Feldkamp-Davis-Kress (FDK), McKinnon-Bates (MKB), or adaptive-steepest-descent projection-onto-convex-sets (ASD-POCS)]. The image quality was quantified using signal-to-noise ratio (SNR), contrast-to-noise ratio, and edge-response width in order to assess noise/streaking and blur. The SNR values were also analyzed with respect to the maximum, mean, and root-mean-squared-error (RMSE) projection angular spacing to investigate how projection angular spacing affects image quality.
Results: The choice of respiratory signals was found to have no significant impact on image quality. Displacement-based binning was found to be less prone to motion artifacts compared to phase binning in more than half of the cases, but was shown to suffer from large interbin image quality variation and large projection angular gaps. Both MKB and ASD-POCS resulted in noticeably improved image quality almost 100% of the time relative to FDK. In addition, SNR values were found to increase with decreasing RMSE values of projection angular gaps with strong correlations (r ≈ -0.7) regardless of the reconstruction algorithm used.
Conclusions: Based on the authors' results, displacement-based binning methods, better reconstruction algorithms, and the acquisition of even projection angular views are the most important factors to consider for improving thoracic 4D-CBCT image quality. In view of the practical issues with displacement-based binning and the fact that projection angular spacing is not currently directly controllable, development of better reconstruction algorithms represents the most effective strategy for improving image quality in thoracic 4D-CBCT for IGRT applications at the current stage.
© 2014 American Association of Physicists in Medicine.
Figures











References
-
- Gierga D. P., Brewer J., Sharp G. C., Betke M., Willett C. G., and Chen G. T. Y., “The correlation between internal and external markers for abdominal tumors: Implications for respiratory gating,” Int. J. Radiat. Oncol., Biol., Phys. 61(5), 1551–1558 (2005).10.1016/j.ijrobp.2004.12.013 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
