

Cardiac arrest during hospitalization for delivery in the United States, 1998-2011
- PMID: 24694844
- PMCID: PMC4445354
- DOI: 10.1097/ALN.0000000000000159
Cardiac arrest during hospitalization for delivery in the United States, 1998-2011
Abstract
Background: The objective of this analysis was to evaluate the frequency, distribution of potential etiologies, and survival rates of maternal cardiopulmonary arrest during the hospitalization for delivery in the United States.
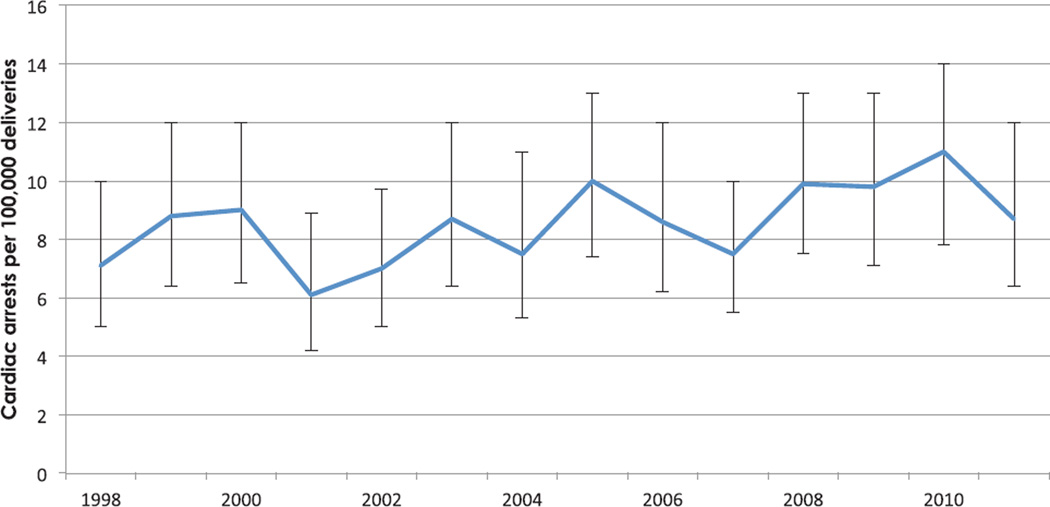
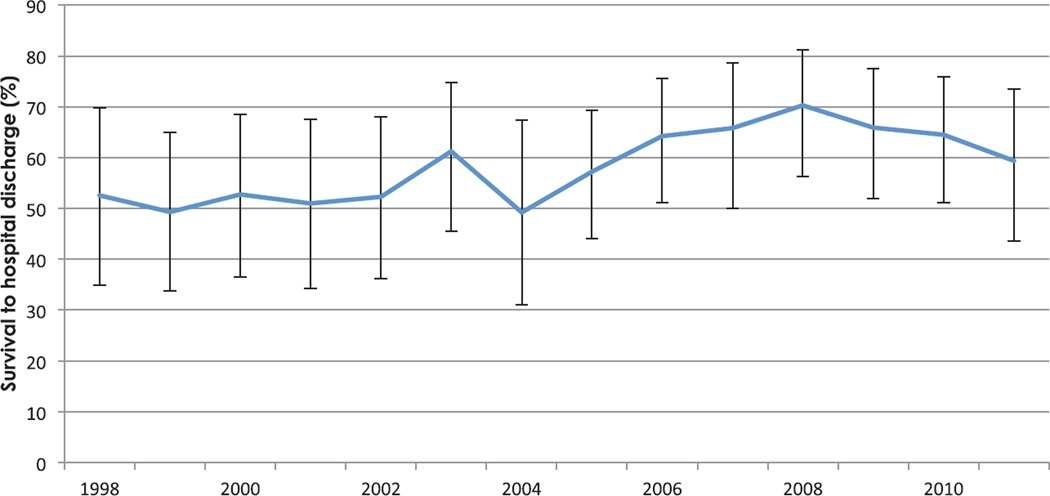
Methods: By using data from the Nationwide Inpatient Sample during the years 1998 through 2011, the authors obtained weighted estimates of the number of U.S. hospitalizations for delivery complicated by maternal cardiac arrest. Clinical and demographic risk factors, potential etiologies, and outcomes were identified and compared in women with and without cardiac arrest. The authors tested for temporal trends in the occurrence and survival associated with maternal arrest.
Results: Cardiac arrest complicated 1 in 12,000 or 8.5 per 100,000 hospitalizations for delivery (99% CI, 7.7 to 9.3 per 100,000). The most common potential etiologies of arrest included hemorrhage, heart failure, amniotic fluid embolism, and sepsis. Among patients with cardiac arrest, 58.9% of patients (99% CI, 54.8 to 63.0%) survived to hospital discharge.
Conclusions: Approximately 1 in 12,000 hospitalizations for delivery is complicated by cardiac arrest, most frequently due to hemorrhage, heart failure, amniotic fluid embolism, or sepsis. Survival depends on the underlying etiology of arrest.
Figures
Comment in
-
Estimating maternal cardiac arrest incidence and outcomes: a rare and challenging complication of pregnancy that behooves preparedness.Anesthesiology. 2014 Apr;120(4):790-1. doi: 10.1097/ALN.0000000000000162. Anesthesiology. 2014. PMID: 24694842 No abstract available.
References
-
- Morrison LJ, Deakin CD, Morley PT, Callaway CW, Kerber RE, Kronick SL, Lavonas EJ, Link MS, Neumar RW, Otto CW, Parr M, Shuster M, Sunde K, Peberdy MA, Tang W, Hoek TL, Böttiger BW, Drajer S, Lim SH, Nolan JP. Advanced Life Support Chapter Collaborators: Part 8: Advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122(16 suppl 2):S345–S421. - PubMed
-
- Kuklina EV, Whiteman MK, Hillis SD, Jamieson DJ, Meikle SF, Posner SF, Marchbanks PA. An enhanced method for identifying obstetric deliveries: Implications for estimating maternal morbidity. Matern Child Health J. 2008;12:469–477. - PubMed
-
- Mhyre JM, Bateman BT, Leffert LR. Influence of patient comorbidities on the risk of near-miss maternal morbidity or mortality. Anesthesiology. 2011;115:963–972. - PubMed
-
- Berg CJ, Callaghan WM, Syverson C, Henderson Z. Pregnancy-related mortality in the United States, 1998 to 2005. Obstet Gynecol. 2010;116:1302–1309. - PubMed
-
- Lennox C, Marr L. Scottish Confidential Audit of Severe Maternal Morbidity 9th Annual Report. Edinburgh, Scotland, Healthcare Improvement Scotland. 2013:1–62.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
