

Validation of the Oxford classification of IgA nephropathy in cohorts with different presentations and treatments
- PMID: 24694989
- PMCID: PMC4184028
- DOI: 10.1038/ki.2014.63
Validation of the Oxford classification of IgA nephropathy in cohorts with different presentations and treatments
Abstract
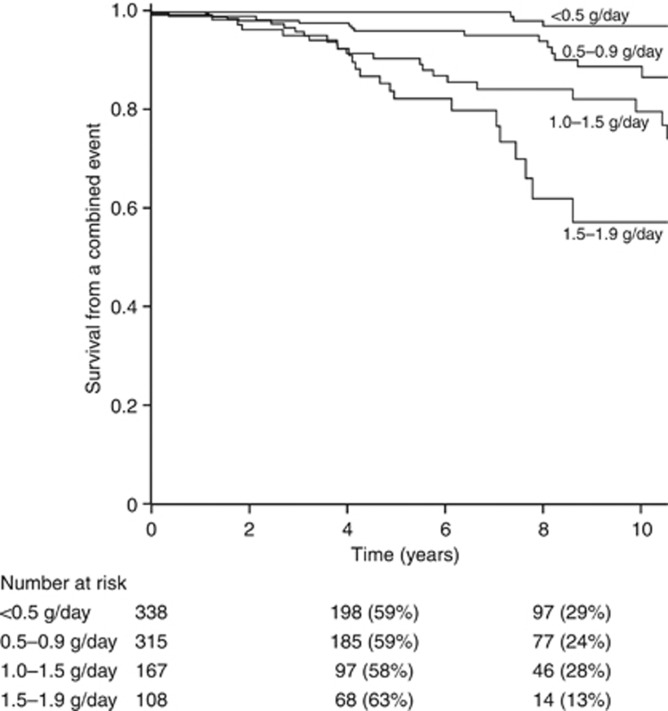
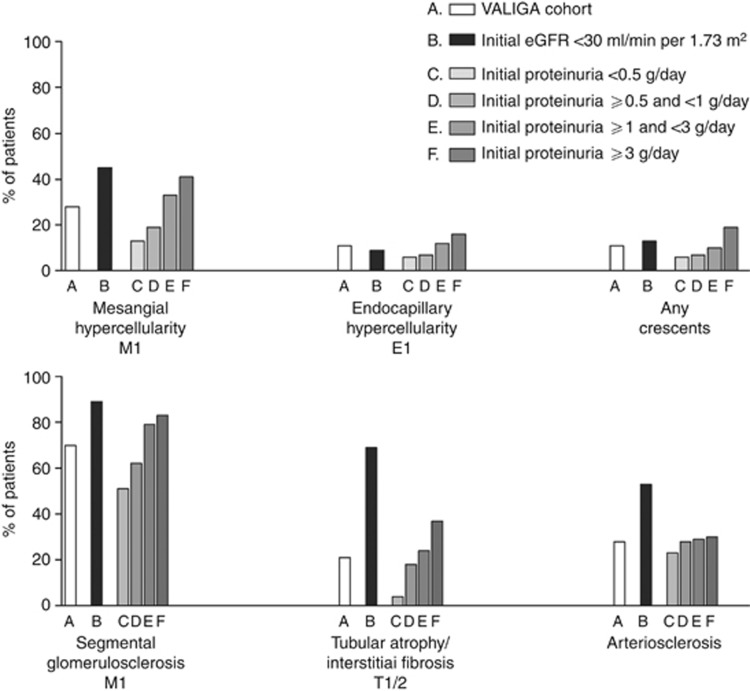
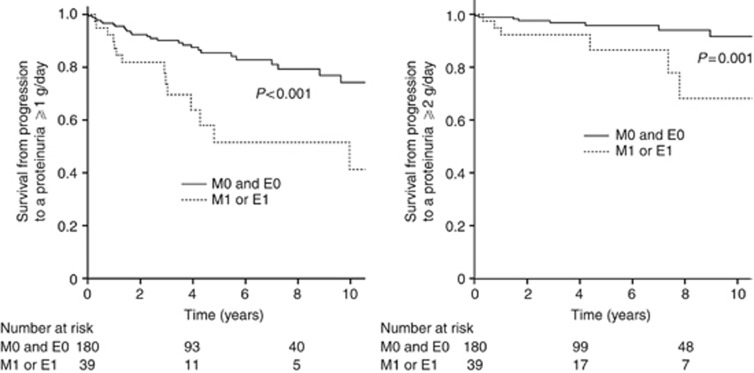
The Oxford Classification of IgA Nephropathy (IgAN) identified mesangial hypercellularity (M), endocapillary proliferation (E), segmental glomerulosclerosis (S), and tubular atrophy/interstitial fibrosis (T) as independent predictors of outcome. Whether it applies to individuals excluded from the original study and how therapy influences the predictive value of pathology remain uncertain. The VALIGA study examined 1147 patients from 13 European countries that encompassed the whole spectrum of IgAN. Over a median follow-up of 4.7 years, 86% received renin-angiotensin system blockade and 42% glucocorticoid/immunosuppressive drugs. M, S, and T lesions independently predicted the loss of estimated glomerular filtration rate (eGFR) and a lower renal survival. Their value was also assessed in patients not represented in the Oxford cohort. In individuals with eGFR less than 30 ml/min per 1.73 m(2), the M and T lesions independently predicted a poor survival. In those with proteinuria under 0.5 g/day, both M and E lesions were associated with a rise in proteinuria to 1 or 2 g/day or more. The addition of M, S, and T lesions to clinical variables significantly enhanced the ability to predict progression only in those who did not receive immunosuppression (net reclassification index 11.5%). The VALIGA study provides a validation of the Oxford classification in a large European cohort of IgAN patients across the whole spectrum of the disease. The independent predictive value of pathology MEST score is reduced by glucocorticoid/immunosuppressive therapy.
Figures
Comment in
-
Toward 100% prediction of progression by fractional excretion of IgG in combination with nephron loss in IgA nephropathy.Kidney Int. 2014 Nov;86(5):1062. doi: 10.1038/ki.2014.247. Kidney Int. 2014. PMID: 25360505 No abstract available.
-
Validation of the Oxford classification of IgA nephropathy: valid or invalid?Kidney Int. 2015 Mar;87(3):661-2. doi: 10.1038/ki.2014.401. Kidney Int. 2015. PMID: 25723637 No abstract available.
-
The authors reply:Kidney Int. 2015 Mar;87(3):662-3. doi: 10.1038/ki.2014.402. Kidney Int. 2015. PMID: 25723639 No abstract available.
References
-
- D'Amico G. The commonest glomerulonephritis in the world: IgA nephropathy. Q J Med. 1987;64:709–727. - PubMed
-
- Zeng CH, Le W, Ni Z, et al. A multicenter application and evaluation of the Oxford classification of IgA nephropathy in adult Chinese patients. Am J Kidney Dis. 2012;60:812–820. - PubMed
-
- Manno C, Strippoli GF, D'Altri C, et al. A novel simpler histological classification for renal survival in IgA nephropathy: a retrospective study. Am J Kidney Dis. 2007;49:763–775. - PubMed
-
- Maixnerova D, Bauerova L, Skibova J, et al. The retrospective analysis of 343 Czech patients with IgA nephropathy: one centre experience. Nephrol Dial Transplant. 2012;27:1492–1498. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
