

Prediction of nodal involvement in primary rectal carcinoma without invasion to pelvic structures: accuracy of preoperative CT, MR, and DWIBS assessments relative to histopathologic findings
- PMID: 24695111
- PMCID: PMC3973633
- DOI: 10.1371/journal.pone.0092779
Prediction of nodal involvement in primary rectal carcinoma without invasion to pelvic structures: accuracy of preoperative CT, MR, and DWIBS assessments relative to histopathologic findings
Abstract
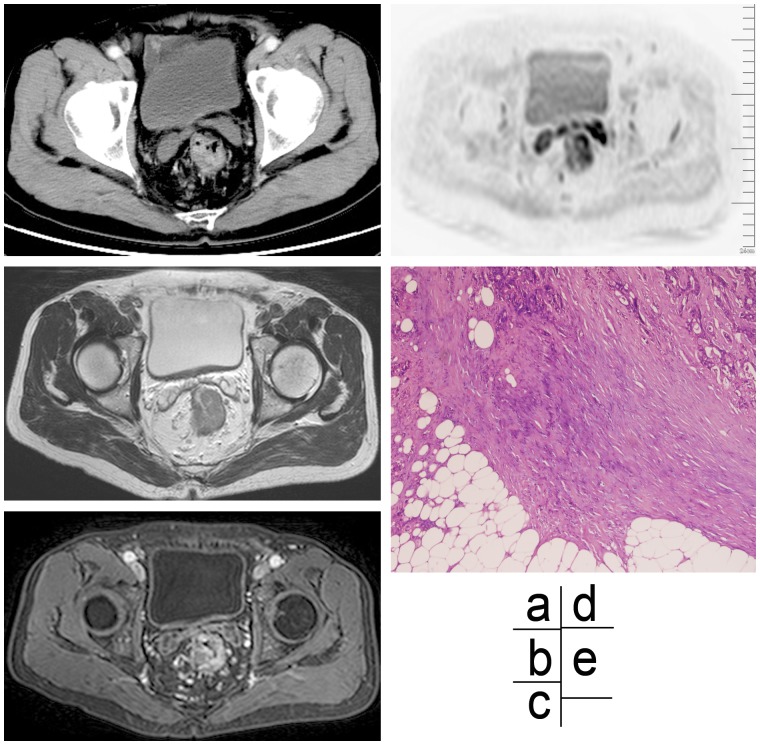
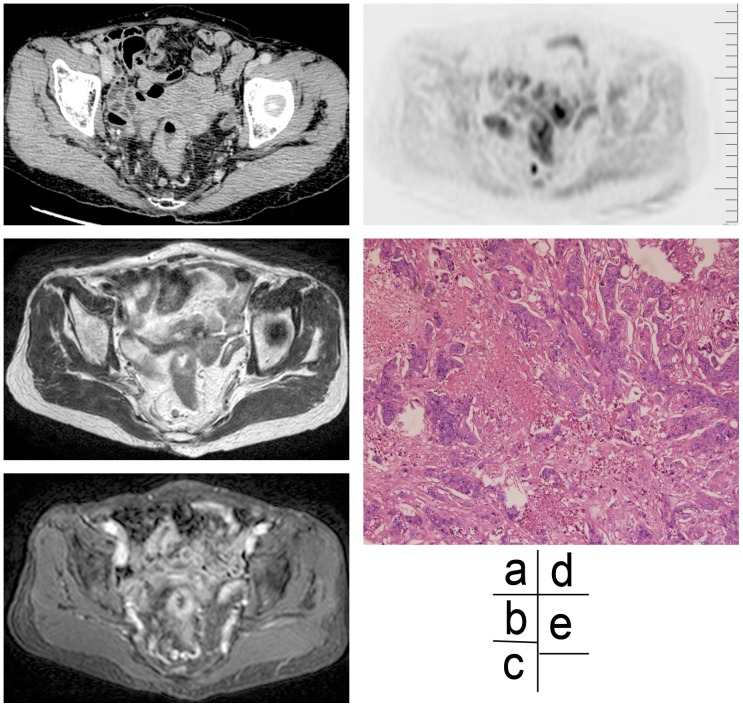
Objective: To investigate the accuracy of preoperative computed tomography (CT), magnetic resonance (MR) imaging and diffusion-weighted imaging with background body signal suppression (DWIBS) in the prediction of nodal involvement in primary rectal carcinoma patients in the absence of tumor invasion into pelvic structures.
Methods and materials: Fifty-two subjects with primary rectal cancer were preoperatively assessed by CT and MRI at 1.5 T with a phased-array coil. Preoperative lymph node staging with imaging modalities (CT, MRI, and DWIBS) were compared with the final histological findings.
Results: The accuracy of CT, MRI, and DWIBS were 57.7%, 63.5%, and 40.4%. The accuracy of DWIBS with higher sensitivity and negative predictive value for evaluating primary rectal cancer patients was lower than that of CT and MRI. Nodal staging agreement between imaging and pathology was fairly strong for CT and MRI (Kappa value = 0.331 and 0.348, P<0.01) but was relatively weaker for DWIBS (Kappa value = 0.174, P<0.05). The accuracy was 57.7% and 59.6%, respectively, for CT and MRI when the lymph node border information was used as the criteria, and was 57.7% and 61.5%, respectively, for enhanced CT and MRI when the lymph node enhancement pattern was used as the criteria.
Conclusion: MRI is more accurate than CT in predicting nodal involvement in primary rectal carcinoma patients in the absence of tumor invasion into pelvic structures. DWIBS has a great diagnostic value in differentiating small malignant from benign lymph nodes.
Conflict of interest statement
Figures

References
-
- Bipat S, Glas AS, Slors FJ, Zwinderman AH, Bossuyt PM, et al. (2004) Rectal Cancer: Local Staging and Assessment of Lymph Node Involvement with Endoluminal US, CT, and MR Imaging–A Meta-Analysis1. Radiology 232: 773–783. - PubMed
-
- Brown G, Richards CJ, Newcombe RG, Dallimore NS, Radcliffe AG, et al. (1999) Rectal Carcinoma: Thin-Section MR Imaging for Staging in 28 Patients1. Radiology 211: 215–222. - PubMed
-
- Wallengren N-O, Holtås S, Andrén-Sandberg Å, Jonsson E, Kristoffersson DT, et al. (2000) Rectal Carcinoma: Double-Contrast MR Imaging for Preoperative Staging1. Radiology 215: 108–114. - PubMed
-
- Lahaye MJ, Engelen SM, Kessels AG, de Bruïne AP, von Meyenfeldt MF, et al. (2008) USPIO-enhanced MR imaging for nodal staging in patients with primary rectal cancer: predictive criteria1. Radiology 246: 804–811. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
