

A new avenue for lithium: intervention in traumatic brain injury
- PMID: 24697257
- PMCID: PMC4063503
- DOI: 10.1021/cn500040g
A new avenue for lithium: intervention in traumatic brain injury
Abstract
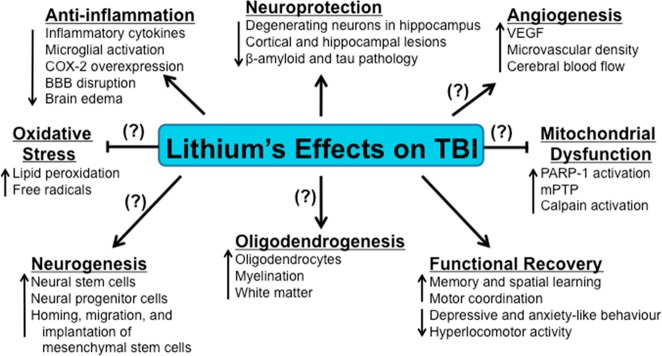
Traumatic brain injury (TBI) is a leading cause of disability and death from trauma to central nervous system (CNS) tissues. For patients who survive the initial injury, TBI can lead to neurodegeneration as well as cognitive and motor deficits, and is even a risk factor for the future development of neurodegenerative disorders such as Alzheimer's disease. Preclinical studies of multiple neuropathological and neurodegenerative disorders have shown that lithium, which is primarily used to treat bipolar disorder, has considerable neuroprotective effects. Indeed, emerging evidence now suggests that lithium can also mitigate neurological deficits incurred from TBI. Lithium exerts neuroprotective effects and stimulates neurogenesis via multiple signaling pathways; it inhibits glycogen synthase kinase-3 (GSK-3), upregulates neurotrophins and growth factors (e.g., brain-derived neurotrophic factor (BDNF)), modulates inflammatory molecules, upregulates neuroprotective factors (e.g., B-cell lymphoma-2 (Bcl-2), heat shock protein 70 (HSP-70)), and concomitantly downregulates pro-apoptotic factors. In various experimental TBI paradigms, lithium has been shown to reduce neuronal death, microglial activation, cyclooxygenase-2 induction, amyloid-β (Aβ), and hyperphosphorylated tau levels, to preserve blood-brain barrier integrity, to mitigate neurological deficits and psychiatric disturbance, and to improve learning and memory outcome. Given that lithium exerts multiple therapeutic effects across an array of CNS disorders, including promising results in preclinical models of TBI, additional clinical research is clearly warranted to determine its therapeutic attributes for combating TBI. Here, we review lithium's exciting potential in ameliorating physiological as well as cognitive deficits induced by TBI.
Keywords: Anti-inflammation; GSK-3 (glycogen synthase kinase-3) inhibitor; TBI (traumatic brain injury); behavioral deficits and cognitive improvements; combined therapy treatment; controlled cortical impact; functional recovery; lithium; mood stabilizer; neuroprotection; neuroregeneration; preclinical model.
Figures
Similar articles
-
Lithium ameliorates neurodegeneration, suppresses neuroinflammation, and improves behavioral performance in a mouse model of traumatic brain injury.J Neurotrauma. 2012 Jan 20;29(2):362-74. doi: 10.1089/neu.2011.1942. Epub 2011 Nov 1. J Neurotrauma. 2012. PMID: 21895523 Free PMC article.
-
Lithium reduces BACE1 overexpression, β amyloid accumulation, and spatial learning deficits in mice with traumatic brain injury.J Neurotrauma. 2012 Sep;29(13):2342-51. doi: 10.1089/neu.2012.2449. Epub 2012 Jul 2. J Neurotrauma. 2012. PMID: 22583494 Free PMC article.
-
Inhibition of Glycogen Synthase Kinase-3: An Emerging Target in the Treatment of Traumatic Brain Injury.J Neurotrauma. 2016 Dec 1;33(23):2065-2076. doi: 10.1089/neu.2015.4177. Epub 2016 May 9. J Neurotrauma. 2016. PMID: 26979735 Review.
-
Elucidating the pivotal molecular mechanisms, therapeutic and neuroprotective effects of lithium in traumatic brain injury.Brain Behav. 2024 Jun;14(6):e3595. doi: 10.1002/brb3.3595. Brain Behav. 2024. PMID: 38874089 Free PMC article. Review.
-
Posttrauma cotreatment with lithium and valproate: reduction of lesion volume, attenuation of blood-brain barrier disruption, and improvement in motor coordination in mice with traumatic brain injury.J Neurosurg. 2013 Sep;119(3):766-73. doi: 10.3171/2013.6.JNS13135. Epub 2013 Jul 12. J Neurosurg. 2013. PMID: 23848820 Free PMC article.
Cited by
-
Recent Advances in Fluorescence Imaging of Traumatic Brain Injury in Animal Models.Front Mol Biosci. 2021 May 26;8:660993. doi: 10.3389/fmolb.2021.660993. eCollection 2021. Front Mol Biosci. 2021. PMID: 34124151 Free PMC article. Review.
-
Frontal Traumatic Brain Injury in Rats Causes Long-Lasting Impairments in Impulse Control That Are Differentially Sensitive to Pharmacotherapeutics and Associated with Chronic Neuroinflammation.ACS Chem Neurosci. 2016 Nov 16;7(11):1531-1542. doi: 10.1021/acschemneuro.6b00166. Epub 2016 Aug 30. ACS Chem Neurosci. 2016. PMID: 27525447 Free PMC article.
-
Glycogen synthase kinase-3 as a therapeutic target for cognitive dysfunction in neuropsychiatric disorders.CNS Drugs. 2015 Jan;29(1):1-15. doi: 10.1007/s40263-014-0213-z. CNS Drugs. 2015. PMID: 25380674 Review.
-
What's New in Traumatic Brain Injury: Update on Tracking, Monitoring and Treatment.Int J Mol Sci. 2015 May 26;16(6):11903-65. doi: 10.3390/ijms160611903. Int J Mol Sci. 2015. PMID: 26016501 Free PMC article. Review.
-
Role of Wnt Signaling in Central Nervous System Injury.Mol Neurobiol. 2016 May;53(4):2297-311. doi: 10.1007/s12035-015-9138-x. Epub 2015 May 15. Mol Neurobiol. 2016. PMID: 25976365 Review.
References
-
- Maas A. I.; Stocchetti N.; Bullock R. (2008) Moderate and severe traumatic brain injury in adults. Lancet Neurol. 7(8), 728–741. - PubMed
-
- Faul M., Xu L., Wald M. M., and Coronado V. G. (2010) Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002–2006, Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Atlanta, GA.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
