

Relationships between A(H1N1)pdm09 influenza infection and infections with other respiratory viruses
- PMID: 24698156
- PMCID: PMC4181801
- DOI: 10.1111/irv.12249
Relationships between A(H1N1)pdm09 influenza infection and infections with other respiratory viruses
Abstract
Background: A(H1N1)pdm09, a new influenza pandemic virus emerged in 2009. The A(H1N1)pdm09 infection had several unique characteristics which included rapid transmissibility and high morbidity in obese individuals, pregnant women and individuals suffering from chronic diseases.
Objectives: To study the relationships between A(H1N1)pdm09 influenza infection and infections with other respiratory viruses such as respiratory syncytial virus (RSV), human metapneumo virus (hMPV), adenovirus and seasonal influenza.
Methods: Samples (nasopharyngeal swabs or aspirates) collected between 2007 until 2012 from patients of various ages that were hospitalized due to respiratory virus infections were analyzed for the presence of various respiratory viruses, using qRT-PCR.
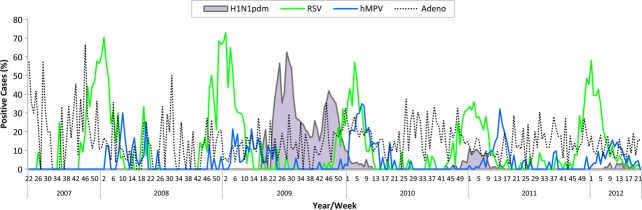
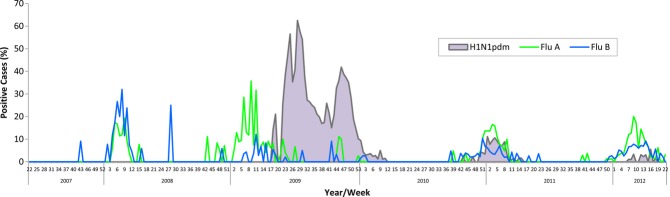
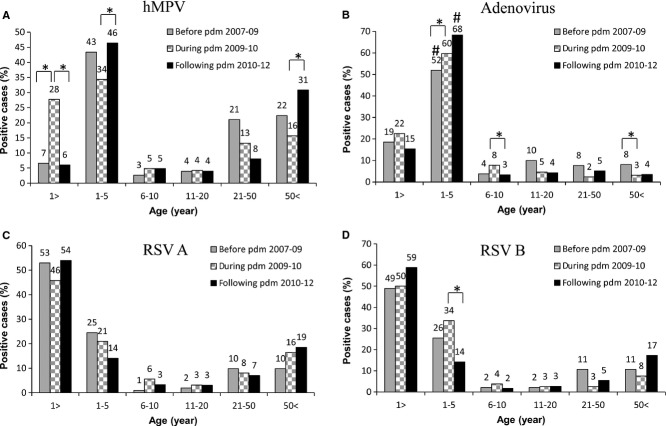
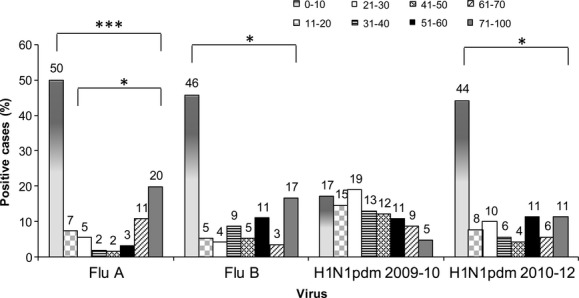
Results: In 2009-2010, when the pandemic influenza A(H1N1)pdm09 first appeared, two major infection peaks were noted and individuals of various ages were infected. Following the decline of the A(H1N1)pdm09 virus infection, the percentages of patients infected with adenovirus and hMPV increased, while infection frequency with RSV B and with seasonal influenza virus decreased. Furthermore, RSV infections were delayed and very few percentages of patients were co-infected with more than one virus. Interestingly, the A(H1N1)pdm09 virus lost its dominancy when it reappeared in the winter of 2010-2011, and at this time, only the incidence of RSV infections was affected by the A(H1N1)pdm09 virus.
Conclusions: The A(H1N1)pdm09 virus had distinct effects on other respiratory viruses when it first appeared versus later, when it evolved from being a pandemic to a seasonal virus.
Keywords: A(H1N1)pdm09 virus; human metapneumo virus; respiratory syncytial virus; respiratory viruses; seasonal influenza viruses.
© 2014 The Authors. Influenza and Other Respiratory Viruses Published by John Wiley & Sons Ltd.
Figures

References
-
- Feuillet F, Lina B, Rosa-Calatrava M, Boivin G. Ten years of human metapneumovirus research. J Clin Virol. 2012;53:97–105. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
