

Evaluation and management of cerebral venous thrombosis
- PMID: 24699485
- PMCID: PMC10564072
- DOI: 10.1212/01.CON.0000446105.67173.a8
Evaluation and management of cerebral venous thrombosis
Abstract
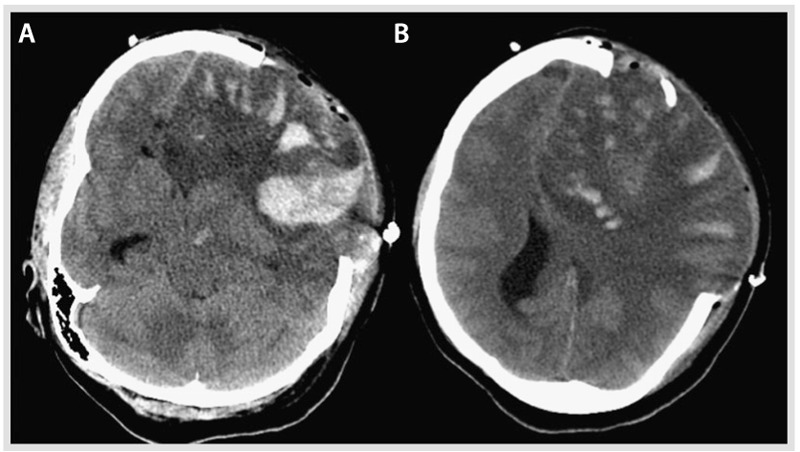
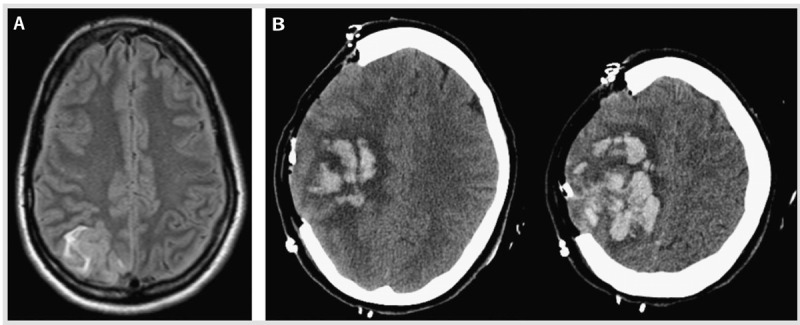
Purpose of review: Thrombosis of the dural sinus and/or cerebral veins (CVT) is a rare but potentially devastating type of stroke that tends to occur in young adults, especially women. In this article, the abbreviation CVT refers to either cerebral venous thrombosis or dural sinus thrombosis. The purpose of this review is to review the most up-to-date literature on the epidemiology, diagnosis, management, and prognosis of CVT. In addition, illustrative cases that represent the spectrum of CVT are provided.
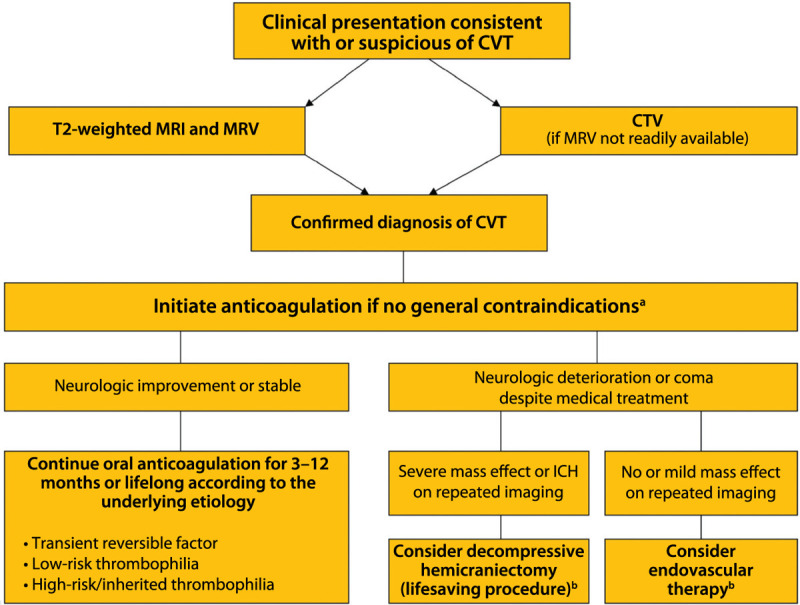
Recent findings: CVT represents about 0.5% of all strokes and can be challenging to diagnose because headache, rather than focal neurologic symptoms, is the prominent feature. The diagnosis is confirmed with MRI and magnetic resonance venogram (MRV). The mainstay of acute management is anticoagulation, although, in the cases of severe hemorrhagic conversion of a venous infarction, endovascular mechanical thrombectomy may be potentially lifesaving. The evaluation of underlying causes from transient triggers, eg, pregnancy, oral contraceptives, or infection, versus chronic triggers, eg, cancer and thrombophilia, will often influence the duration of anticoagulation. The outcomes after CVT are generally favorable, and the risk of recurrence is low.
Summary: CVT is an important diagnosis to keep in mind when evaluating patients with headache in the emergency department, and it is important that it not be overlooked because it is treatable.
Figures
References
-
- Bousser MG,, Ferro JM. Cerebral venous thrombosis: an update. Lancet Neurol 2007; 6 (2): 162–170. - PubMed
-
- Ferro J,, Canhao P,, Stam J, et al Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke 2004; 35 (3): 664–670. - PubMed
-
- deVeber G,, Andrew M,, Adams C, et al Cerebral sinovenous thrombosis in children. N Engl J Med 2001; 345 (6): 417–423. - PubMed
-
- Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med 2005; 352 (17): 1791–1798. - PubMed
-
- Crassard I,, Bousser MG. Headache in patients with cerebral venous thrombosis [in French]. Rev Neurol (Paris) 2005; 161 (6–7): 706–708. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials