

B-mode ultrasound assessment of diaphragm structure and function in patients with COPD
- PMID: 24700122
- PMCID: PMC4151360
- DOI: 10.1378/chest.13-2306
B-mode ultrasound assessment of diaphragm structure and function in patients with COPD
Abstract
Background: Electromyographic evaluation of diaphragmatic neuromuscular disease in patients with COPD is technically difficult and potentially high risk. Defining standard values for diaphragm thickness and thickening ratio using B-mode ultrasound may provide a simpler, safer means of evaluating these patients.
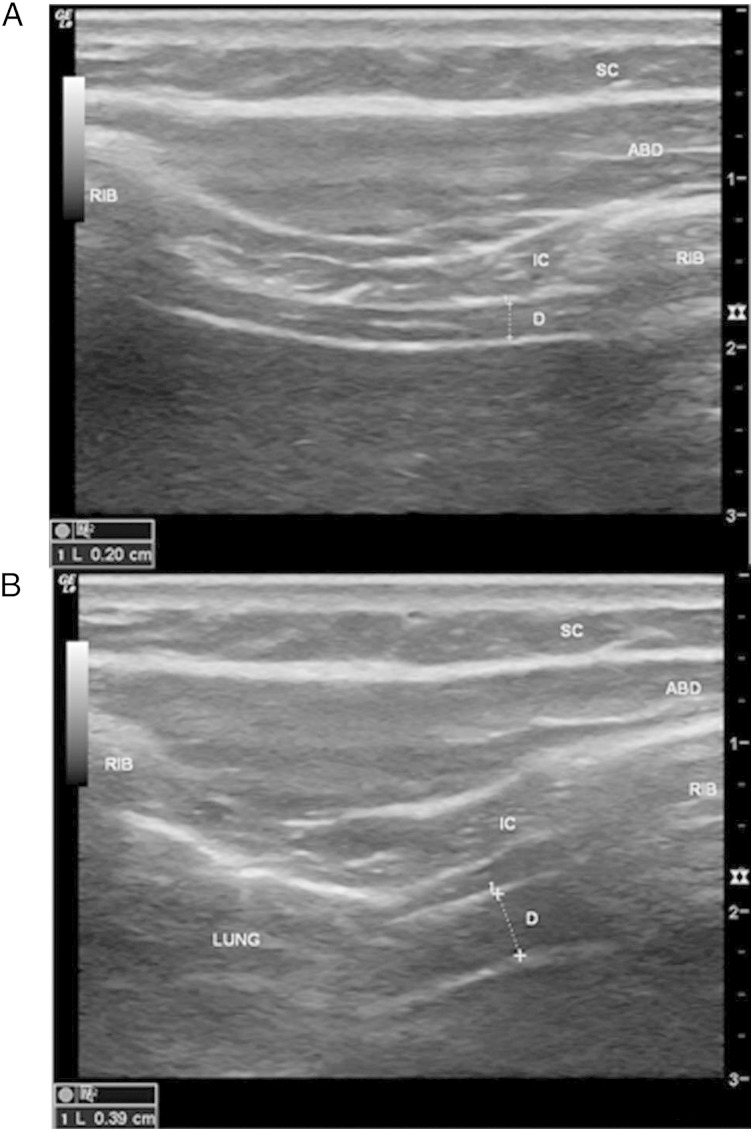
Methods: Fifty patients with a diagnosis of COPD and FEV₁ < 70% underwent B-mode ultrasound. Three images were captured both at end expiration (Tmin) and at maximal inspiration (Tmax). The thickening ratio was calculated as (Tmax/Tmin), and each set of values was averaged. Findings were compared with a database of 150 healthy control subjects.
Results: There was no significant difference in diaphragm thickness or thickening ratio between sides within groups (control subjects or patients with COPD) or between groups, with the exception of the subgroup with severe air trapping (residual volume > 200%), in which the only difference was that the thickening ratio was higher on the left (P = .0045).
Conclusions: In patients with COPD presenting for evaluation of coexisting neuromuscular respiratory weakness, the same values established for healthy control subjects serve as the baseline for comparison. This knowledge expands the role of ultrasound in evaluating neuromuscular disease in patients with COPD.
Figures
Comment in
-
Ultrasound assessment of the diaphragm in patients with COPD.Chest. 2014 Oct;146(4):e146. doi: 10.1378/chest.14-1095. Chest. 2014. PMID: 25288011 No abstract available.
-
Response.Chest. 2014 Oct;146(4):e146-8. doi: 10.1378/chest.14-1228. Chest. 2014. PMID: 25288012 No abstract available.
References
-
- Bolton CF, Grand’Maison F, Parkes A, Shkrum M. Needle electromyography of the diaphragm. Muscle Nerve. 1992;15(6):678-681. - PubMed
-
- Chen R, Collins S, Remtulla H, Parkes A, Bolton CF. Phrenic nerve conduction study in normal subjects. Muscle Nerve. 1995;18(3):330-335. - PubMed
-
- Resman-Gaspersc A, Podnar S. Phrenic nerve conduction studies: technical aspects and normative data. Muscle Nerve. 2008;37(1):36-41. - PubMed
-
- Boon AJ, Alsharif KI, Harper CM, Smith J. Ultrasound-guided needle EMG of the diaphragm: technique description and case report. Muscle Nerve. 2008;38(6):1623-1626. - PubMed
-
- Gerscovich EO, Cronan M, McGahan JP, Jain K, Jones CD, McDonald C. Ultrasonographic evaluation of diaphragmatic motion. J Ultrasound Med. 2001;20(6):597-604. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
