

Normothermic central hypovolemia tolerance reflects hyperthermic tolerance
- PMID: 24700256
- PMCID: PMC4948742
- DOI: 10.1007/s10286-014-0237-y
Normothermic central hypovolemia tolerance reflects hyperthermic tolerance
Abstract
Purpose: To test the hypothesis that those who are highly tolerant to lower body negative pressure (LBNP) while normothermic are also highly tolerant to this challenge while hyperthermic.
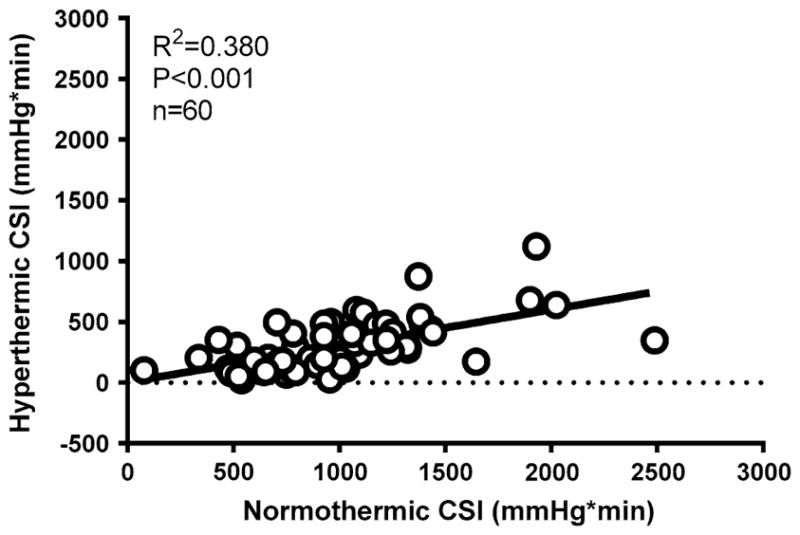
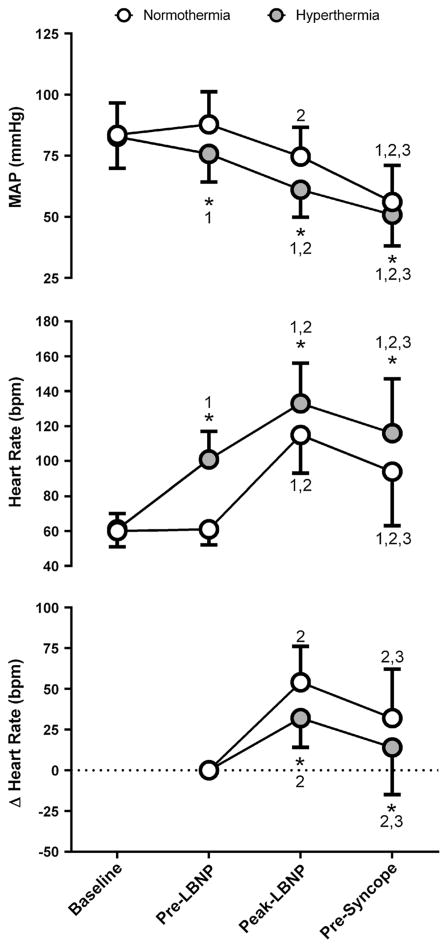
Methods: Sixty pairs of normothermic and hyperthermic LBNP tests to pre-syncope were evaluated. LBNP tolerance was quantified via the cumulative stress index (CSI), which is calculated as the sum of the product of the LBNP level and the duration of each level until test termination (i.e., 20 mmHg × 3 min + 30 mmHg × 3 min, etc.). CSI was compared between normothermic and hyperthermic trials. Internal and skin temperatures, heart rate, and arterial pressure were measured throughout.
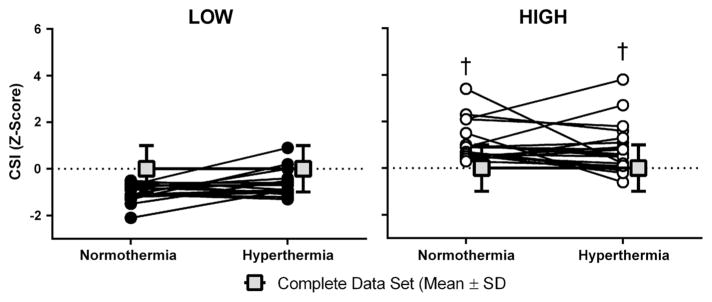
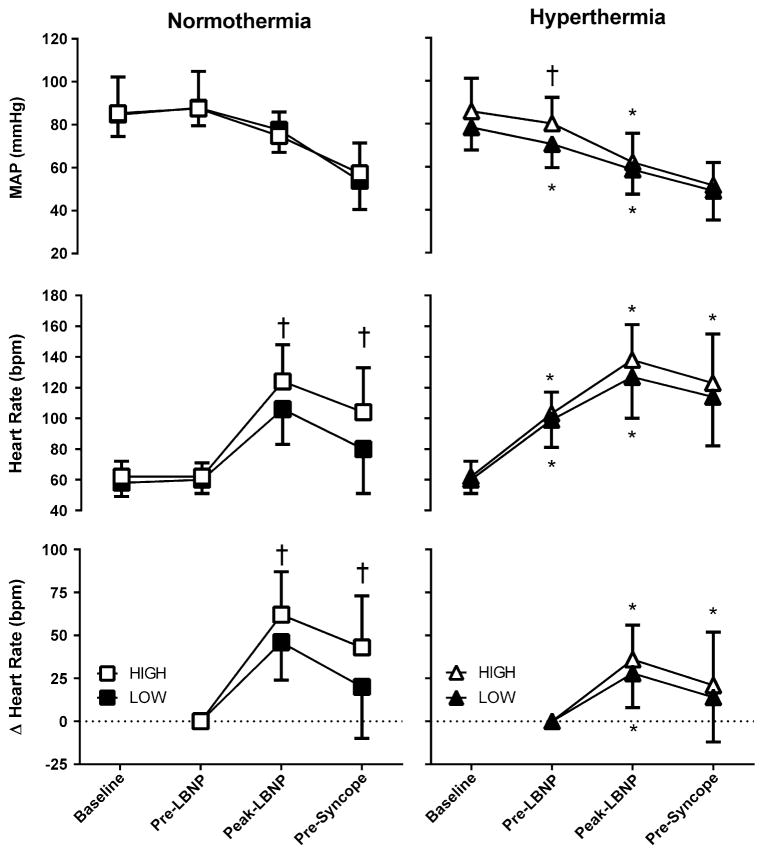
Results: Hyperthermia reduced (P < 0.001) CSI from 997 ± 437 to 303 ± 213 mmHg min. There was a positive correlation between normothermic and hyperthermic LBNP tolerance (R (2) = 0.38; P < 0.001). As a secondary analysis, the 20 trials with the highest LBNP tolerance while normothermic were identified (indicated as the HIGH group; CSI 1,467 ± 356 mmHg min), as were the 20 trials with the lowest normothermic tolerance (indicated as the LOW group; CSI 565 ± 166 mmHg min; P < 0.001 between groups). While hyperthermia unanimously reduced CSI in both HIGH and LOW groups, in this hyperthermic condition CSI was ~threefold higher in the HIGH group (474 ± 226 mmHg min) relative to the LOW group (160 ± 115 mmHg min; P < 0.001).
Conclusions: LBNP tolerance while hyperthermic is related to normothermic tolerance and, associated with this finding, those who have a high LBNP tolerance while normothermic remain relatively tolerant when hyperthermic.
Conflict of interest statement
There are no known conflicts of interest.
Figures
References
-
- Aratow M, Fortney SM, Watenpaugh DE, Crenshaw AG, Hargens AR. Transcapillary fluid responses to lower body negative pressure. J Appl Physiol (1985) 1993;74:2763–2770. - PubMed
-
- Brake DJ, Bates GP. Deep body core temperatures in industrial workers under thermal stress. J Occup Environ Med. 2002;44:125–135. - PubMed
-
- Buller MJ, Welles AP, Stower J, Desantis C, Margolis L, Karis AJ, Economos D, Hoyt RW, Richter MW. Thermal work strain during marine rifle squad operations in Afghanistan (March 2010) USARIEM Technical Report 2010 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
