

Diffusion-weighted MRI for staging and evaluation of response in diffuse large B-cell lymphoma: a pilot study
- PMID: 24700565
- PMCID: PMC4026031
- DOI: 10.1002/nbm.3105
Diffusion-weighted MRI for staging and evaluation of response in diffuse large B-cell lymphoma: a pilot study
Abstract
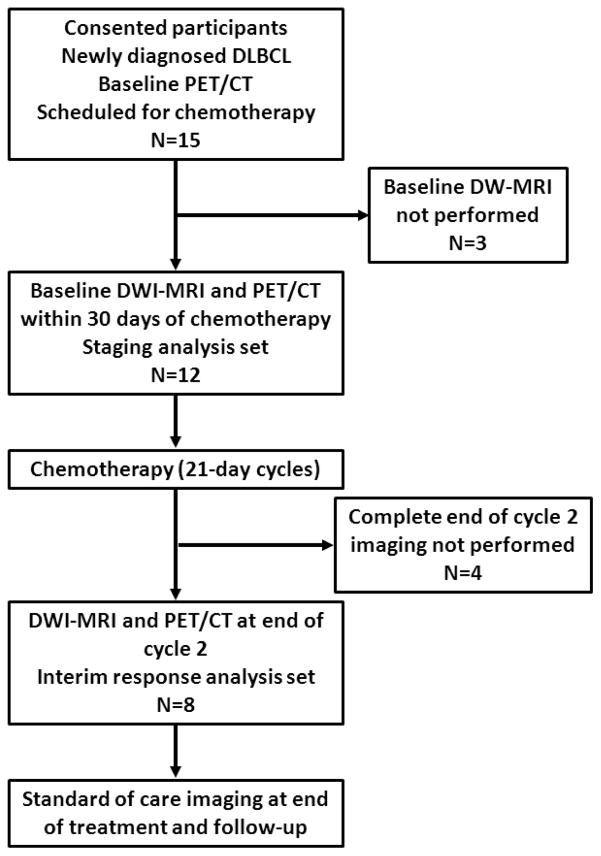
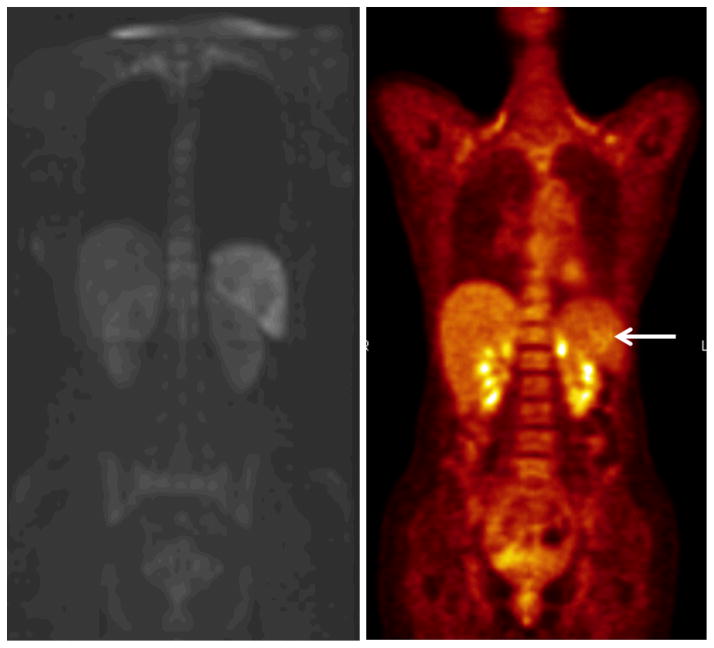
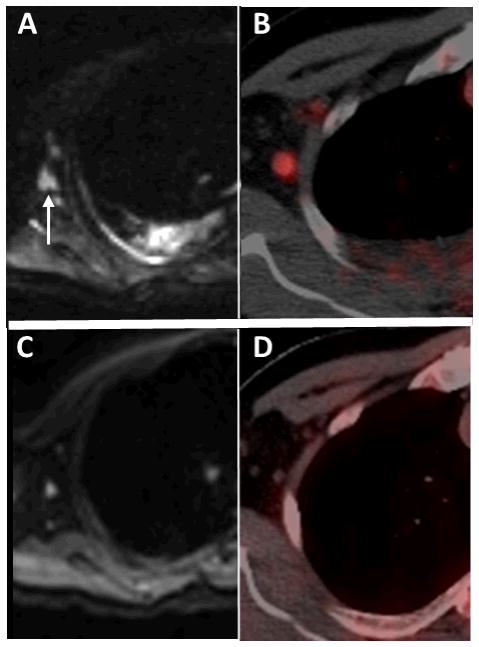
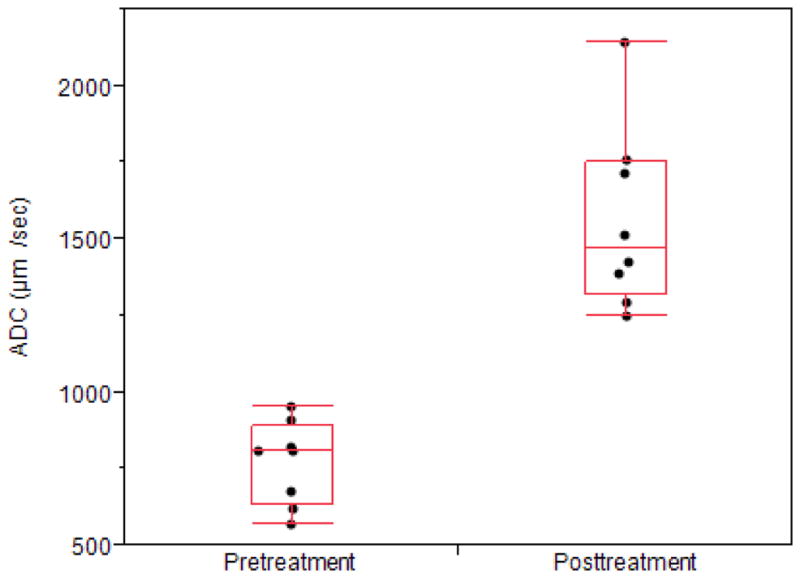
The aim of this study was to compare diffusion-weighted MRI (DW-MRI) with positron emission tomography/computed tomography (PET/CT) for the staging and evaluation of the treatment response in patients with diffuse large B-cell lymphoma (DLBCL). Institutional review board approval was obtained for this study; all subjects gave informed consent. Twelve patients were imaged before treatment and eight of these were also imaged after two cycles of chemotherapy using both DW-MRI and PET/CT. Up to six target lesions were selected at baseline for response assessment based on International Working Group criteria (nodes > 1.5 cm in diameter; extranodal lesions > 1 cm in diameter). For pretreatment staging, visual analysis of the numbers of nodal and extranodal lesions based on PET/CT was performed. For interim response assessment after cycle 2 of chemotherapy, residual tumor sites were assessed visually and the percentage changes in target lesion size, maximum standardized uptake value (SUVmax ) and apparent diffusion coefficient (ADC) from pretreatment values were calculated. In 12 patients studied pretreatment, there were 46 nodal and 16 extranodal sites of lymphomatous involvement. Agreement between DW-MRI and PET/CT for overall lesion detection was 97% (60/62 tumor sites; 44/46 nodal and 16/16 extranodal lesions) and, for Ann Arbor stage, it was 100%. In the eight patients who had interim assessment, five of their 49 tumor sites remained abnormal on visual analysis of both DW-MRI and PET/CT, and there was one false positive on DW-MRI. Of their 24 target lesions, the mean pretreatment ADC value, tumor size and SUVmax were 772 µm(2) /s, 21.3 cm(2) and 16.9 g/mL, respectively. At interim assessment of the same 24 target lesions, ADC values increased by 85%, tumor size decreased by 74% and SUVmax decreased by 83% (all p < 0.01 versus baseline). DW-MRI provides results comparable with those of PET/CT for staging and early response assessment in patients with DLBCL.
Keywords: apparent diffusion coefficient; diffuse large B-cell lymphoma; diffusion-weighted MRI; positron emission tomography/computed tomography (PET/CT); response to chemotherapy; standardized uptake value.
Copyright © 2014 John Wiley & Sons, Ltd.
Figures
Similar articles
-
Diffusion-weighted MRI in early chemotherapy response evaluation of patients with diffuse large B-cell lymphoma--a pilot study: comparison with 2-deoxy-2-fluoro- D-glucose-positron emission tomography/computed tomography.NMR Biomed. 2011 Dec;24(10):1181-90. doi: 10.1002/nbm.1689. Epub 2011 Mar 8. NMR Biomed. 2011. PMID: 21387451 Clinical Trial.
-
Comparison of PET/MRI With PET/CT in the Evaluation of Disease Status in Lymphoma.Clin Nucl Med. 2017 Jan;42(1):e1-e7. doi: 10.1097/RLU.0000000000001344. Clin Nucl Med. 2017. PMID: 27607161 Free PMC article.
-
Whole-Body Diffusion-Weighted MRI Compared to 18 FFDG PET/CT in Initial Staging and Therapy Response Assessment of Hodgkin Lymphoma in Pediatric Patients.Can Assoc Radiol J. 2020 May;71(2):217-225. doi: 10.1177/0846537119888380. Epub 2020 Jan 22. Can Assoc Radiol J. 2020. PMID: 32062992
-
Whole-Body Diffusion-weighted Imaging in Hodgkin Lymphoma and Diffuse Large B-Cell Lymphoma.Radiographics. 2015 May-Jun;35(3):747-64. doi: 10.1148/rg.2015140145. Epub 2015 Mar 27. Radiographics. 2015. PMID: 25815803 Review.
-
18F-FDG PET/CT in the diagnosis of an extranodal relapse of diffuse large B-cell lymphoma (DLBCL): a clinical case with a literature review.Nucl Med Rev Cent East Eur. 2016;19(B):11-13. doi: 10.5603/NMR.2016.0029. Nucl Med Rev Cent East Eur. 2016. PMID: 27813622 Review.
Cited by
-
Detection of bone marrow metastases in children and young adults with solid cancers with diffusion-weighted MRI.Skeletal Radiol. 2023 Jun;52(6):1179-1192. doi: 10.1007/s00256-022-04240-0. Epub 2022 Nov 28. Skeletal Radiol. 2023. PMID: 36441237 Free PMC article.
-
Whole-Body MRI Is an Effective Imaging Modality for Hematological Malignancy Treatment Response Assessment: A Systematic Review and Meta-Analysis.Front Oncol. 2022 Feb 18;12:827777. doi: 10.3389/fonc.2022.827777. eCollection 2022. Front Oncol. 2022. PMID: 35251996 Free PMC article.
-
One-stop local and whole-body staging of children with cancer.Pediatr Radiol. 2022 Feb;52(2):391-400. doi: 10.1007/s00247-021-05076-x. Epub 2021 Apr 30. Pediatr Radiol. 2022. PMID: 33929564 Free PMC article. Review.
-
Therapy Response Assessment of Pediatric Tumors with Whole-Body Diffusion-weighted MRI and FDG PET/MRI.Radiology. 2020 Jul;296(1):143-151. doi: 10.1148/radiol.2020192508. Epub 2020 May 5. Radiology. 2020. PMID: 32368961 Free PMC article.
-
Comparison of diffusion-weighted MRI and [18F]FDG PET/MRI for treatment monitoring in pediatric Hodgkin and non-Hodgkin lymphoma.Eur Radiol. 2024 Jan;34(1):643-653. doi: 10.1007/s00330-023-10015-5. Epub 2023 Aug 5. Eur Radiol. 2024. PMID: 37542653 Free PMC article. Review.
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Juweid ME, Cheson BD. Role of positron emission tomography in lymphoma. J Clin Oncol. 2005;23:4577–4580. - PubMed
-
- Juweid ME, Cheson BD. Positron-emission tomography and assessment of cancer therapy. N Engl J Med. 2006;254:496–507. - PubMed
-
- Kwee TC, Kwee RM, Nievelstein RA. Imaging in staging of malignant lymphoma: a systematic review. Blood. 2008;111:504–516. - PubMed
-
- Shankar LK, Hoffman JM, Bacharach S, Graham MM, Karp J, Lammertsma A, Larson S, Mankoff DA, Siegel BA, Van den Abeele A, Yap J, Sullivan D. Consensus recommendations for the use of 18F-FDG PET as an indicator of therapeutic response in patients in National Cancer Institute trials. J Nucl Med. 2006;47:1059–1066. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
