

Preoperative gadoxetic Acid-enhanced MRI and simultaneous treatment of early hepatocellular carcinoma prolonged recurrence-free survival of progressed hepatocellular carcinoma patients after hepatic resection
- PMID: 24701029
- PMCID: PMC3950411
- DOI: 10.1155/2014/641685
Preoperative gadoxetic Acid-enhanced MRI and simultaneous treatment of early hepatocellular carcinoma prolonged recurrence-free survival of progressed hepatocellular carcinoma patients after hepatic resection
Abstract
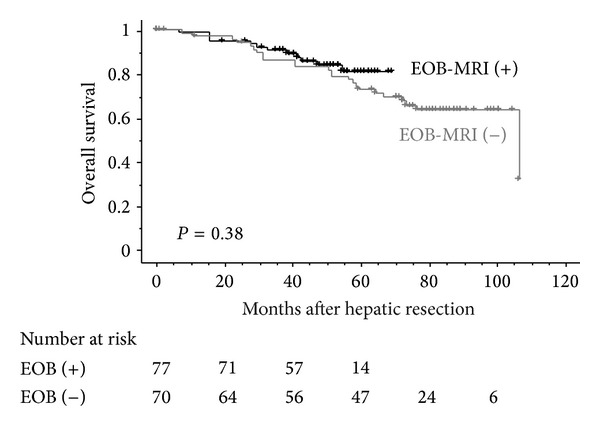
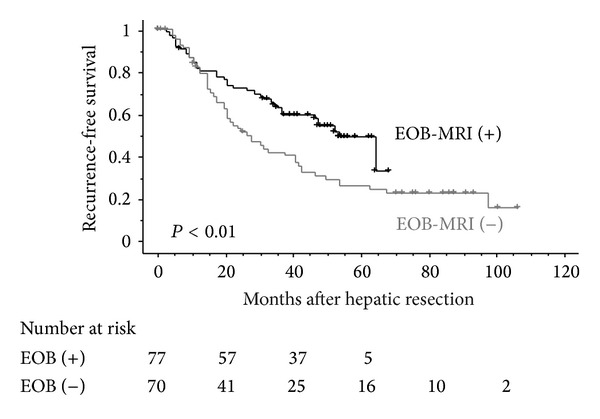
Background/Purpose. The purpose of this study was to clarify whether preoperative gadoxetic acid-enhanced magnetic resonance imaging (EOB-MRI) and simultaneous treatment of suspected early hepatocellular carcinoma (eHCC) at the time of resection for progressed HCC affected patient prognosis following hepatic resection. Methods. A total of 147 consecutive patients who underwent their first curative hepatic resection for progressed HCC were enrolled. Of these, 77 patients underwent EOB-MRI (EOB-MRI (+)) before hepatic resection and the remaining 70 patients did not (EOB-MRI (-)). Suspected eHCCs detected by preoperative imaging were resected or ablated at the time of resection for progressed HCC. Results. The number of patients who underwent treatment for eHCCs was significantly higher in the EOB-MRI (+) than in the EOB-MRI (-) (17 versus 6; P = 0.04). Recurrence-free survival (1-, 3-, and 5-year; 81.4, 62.6, 48.7% versus 82.1, 41.5, 25.5%, resp., P < 0.01), but not overall survival (1-, 3-, and 5-year; 98.7, 90.7, 80.8% versus 97.0, 86.3, 72.4%, resp., P = 0.38), was significantly better in the EOB-MRI (+). Univariate and multivariate analyses showed that preoperative EOB-MRI was one of the independent factors significantly correlated with better recurrence-free survival. Conclusions. Preoperative EOB-MRI and simultaneous treatment of eHCC prolonged recurrence-free survival after hepatic resection.
Figures
Similar articles
-
Clinical value of gadoxetic acid-enhanced magnetic resonance imaging in surgery for hepatocellular carcinoma - with a special emphasis on early hepatocellular carcinoma.World J Hepatol. 2015 Dec 28;7(30):2933-9. doi: 10.4254/wjh.v7.i30.2933. World J Hepatol. 2015. PMID: 26730272 Free PMC article.
-
Performance of gadoxetic acid MRI and diffusion-weighted imaging for the diagnosis of early recurrence of hepatocellular carcinoma.Eur Radiol. 2020 Jan;30(1):186-194. doi: 10.1007/s00330-019-06351-0. Epub 2019 Aug 1. Eur Radiol. 2020. PMID: 31372783
-
Clinical Impact of Gadoxetic Acid-Enhanced Magnetic Resonance Imaging on Hepatoma Management: A Prospective Study.Dig Dis Sci. 2016 Apr;61(4):1197-205. doi: 10.1007/s10620-015-3989-x. Epub 2015 Dec 14. Dig Dis Sci. 2016. PMID: 26668057
-
Diagnostic performance of MRI using extracellular contrast agents versus gadoxetic acid for hepatocellular carcinoma: A systematic review and meta-analysis.Liver Int. 2021 May;41(5):1117-1128. doi: 10.1111/liv.14850. Epub 2021 Mar 8. Liver Int. 2021. PMID: 33647177
-
Focal lesions in the cirrhotic liver: their pivotal role in gadoxetic acid-enhanced MRI and recognition by the Western guidelines.Dig Dis. 2014;32(6):696-704. doi: 10.1159/000368002. Epub 2014 Oct 29. Dig Dis. 2014. PMID: 25376286 Review.
Cited by
-
The Effect of New Therapeutic and Diagnostic Agents on the Prognosis of Hepatocellular Carcinoma in Japan – An Analysis of Data from the Kanagawa Cancer Registry.Asian Pac J Cancer Prev. 2017 Sep 27;18(9):2471-2476. doi: 10.22034/APJCP.2017.18.9.2471. Asian Pac J Cancer Prev. 2017. PMID: 28952279 Free PMC article.
-
Clinical value of gadoxetic acid-enhanced magnetic resonance imaging in surgery for hepatocellular carcinoma - with a special emphasis on early hepatocellular carcinoma.World J Hepatol. 2015 Dec 28;7(30):2933-9. doi: 10.4254/wjh.v7.i30.2933. World J Hepatol. 2015. PMID: 26730272 Free PMC article.
-
Diagnosis of Hepatocellular Carcinoma with Gadoxetic Acid-Enhanced MRI: 2016 Consensus Recommendations of the Korean Society of Abdominal Radiology.Korean J Radiol. 2017 May-Jun;18(3):427-443. doi: 10.3348/kjr.2017.18.3.427. Epub 2017 Apr 3. Korean J Radiol. 2017. PMID: 28458595 Free PMC article. Review.
-
Non-Hypervascular Hypointense Nodules at Gadoxetic Acid MRI: Hepatocellular Carcinoma Risk Assessment with Emphasis on the Role of Diffusion-Weighted Imaging.J Gastrointest Cancer. 2018 Sep;49(3):302-310. doi: 10.1007/s12029-017-9952-7. J Gastrointest Cancer. 2018. PMID: 28547117
-
JSH Consensus-Based Clinical Practice Guidelines for the Management of Hepatocellular Carcinoma: 2014 Update by the Liver Cancer Study Group of Japan.Liver Cancer. 2014 Oct;3(3-4):458-68. doi: 10.1159/000343875. Liver Cancer. 2014. PMID: 26280007 Free PMC article. Review.
References
-
- Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. Journal of Hepatology. 2003;38(2):200–207. - PubMed
-
- Takayama T. Surgical treatment for hepatocellular carcinoma. Japanese Journal of Clinical Oncology. 2011;41(4):447–454.hyr016 - PubMed
-
- Matsuda M, Fujii H, Kono H, Matsumoto Y. Surgical treatment of recurrent hepatocellular carcinoma based on the mode of recurrence: repeat hepatic resection or ablation are good choices for patients with recurrent multicentric cancer. Journal of Hepato-Biliary-Pancreatic Surgery. 2001;8(4):353–359. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources