

A novel non-rapid-eye movement and rapid-eye-movement parasomnia with sleep breathing disorder associated with antibodies to IgLON5: a case series, characterisation of the antigen, and post-mortem study
- PMID: 24703753
- PMCID: PMC4104022
- DOI: 10.1016/S1474-4422(14)70051-1
A novel non-rapid-eye movement and rapid-eye-movement parasomnia with sleep breathing disorder associated with antibodies to IgLON5: a case series, characterisation of the antigen, and post-mortem study
Erratum in
- Lancet Neurol. 2015 Jan;14(1):28
Abstract
Background: Autoimmunity might be associated with or implicated in sleep and neurodegenerative disorders. We aimed to describe the features of a novel neurological syndrome associated with prominent sleep dysfunction and antibodies to a neuronal antigen.
Methods: In this observational study, we used clinical and video polysomnography to identify a novel sleep disorder in three patients referred to the Sleep Unit of Hospital Clinic, University of Barcelona, Spain, for abnormal sleep behaviours and obstructive sleep apnoea. These patients had antibodies against a neuronal surface antigen, which were also present in five additional patients referred to our laboratory for antibody studies. These five patients had been assessed with polysomnography, which was done in our sleep unit in one patient and the recording reviewed in a second patient. Two patients underwent post-mortem brain examination. Immunoprecipitation and mass spectrometry were used to characterise the antigen and develop an assay for antibody testing. Serum or CSF from 298 patients with neurodegenerative, sleep, or autoimmune disorders served as control samples.
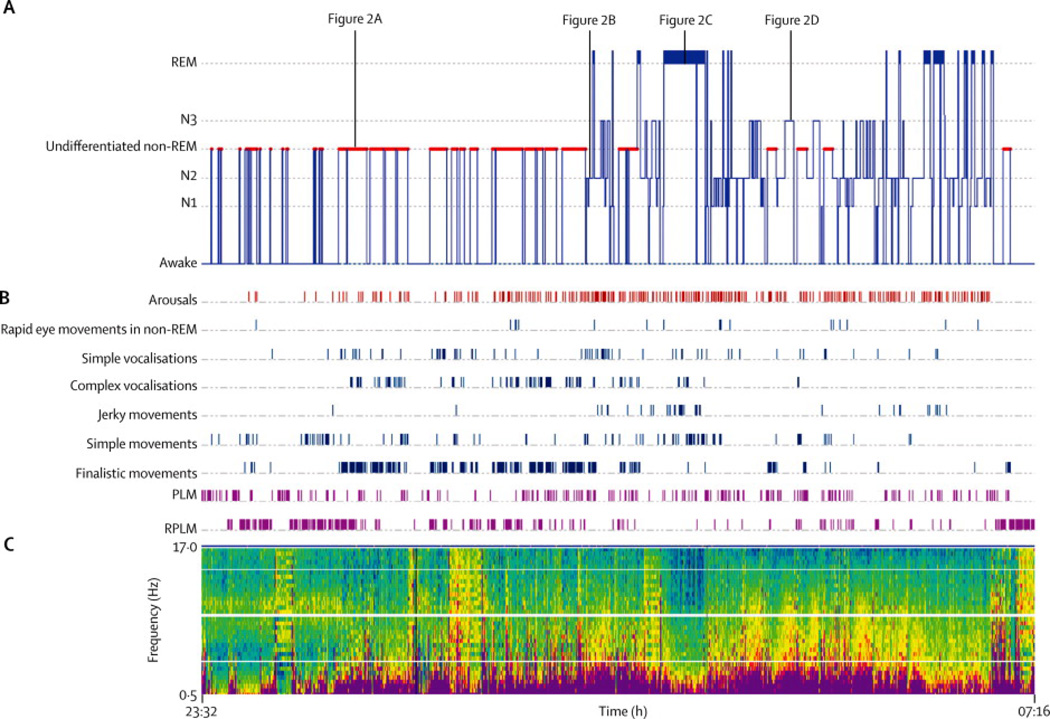
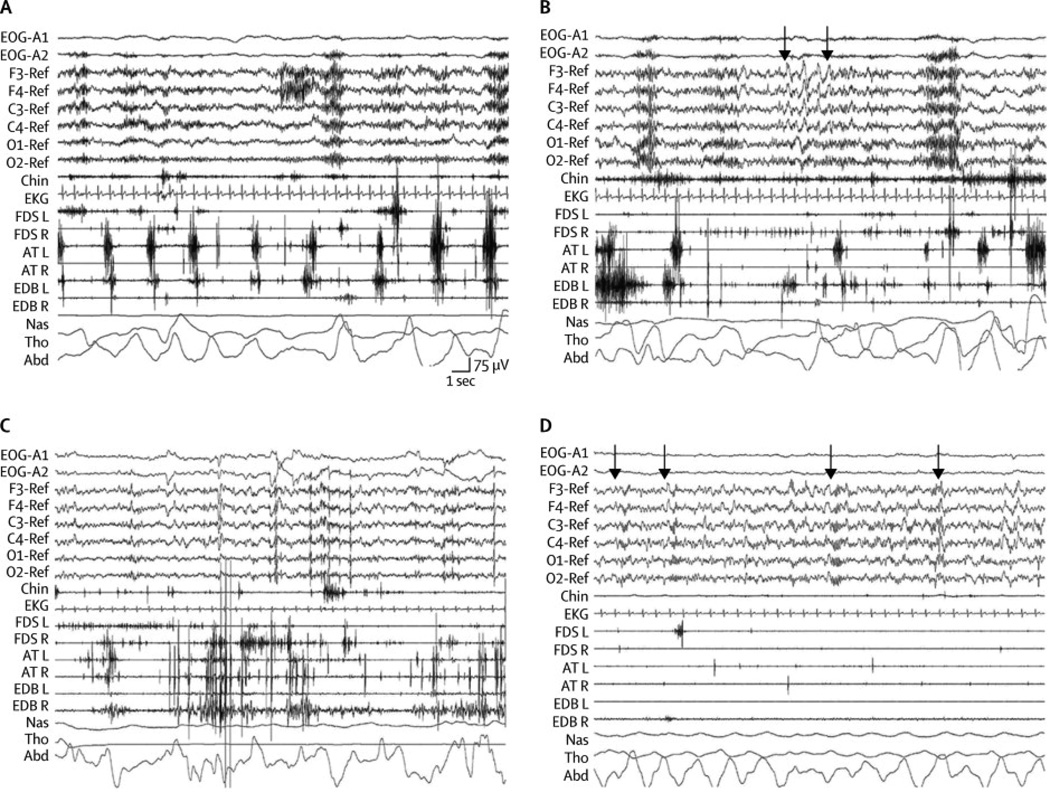
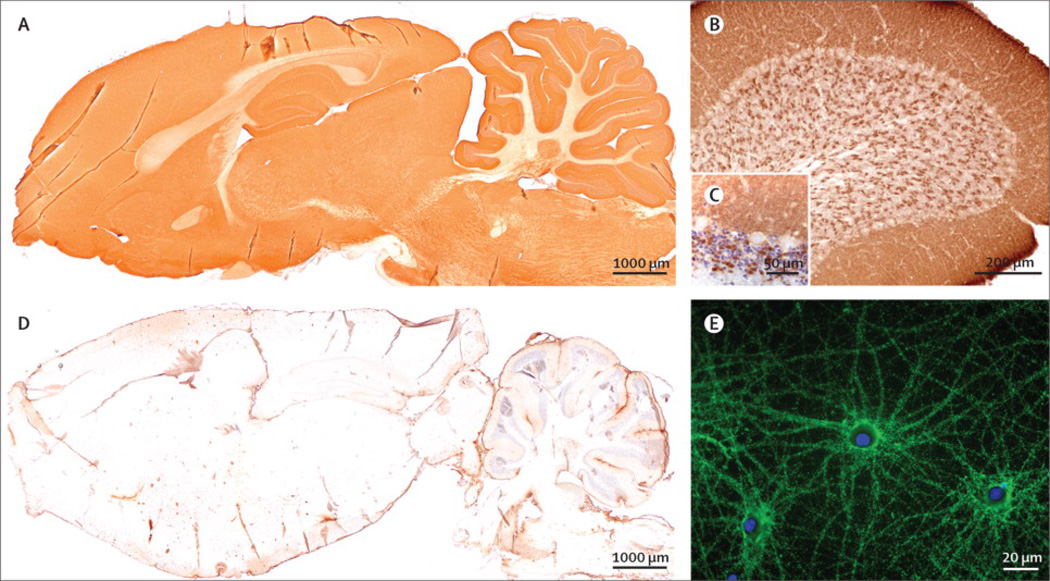
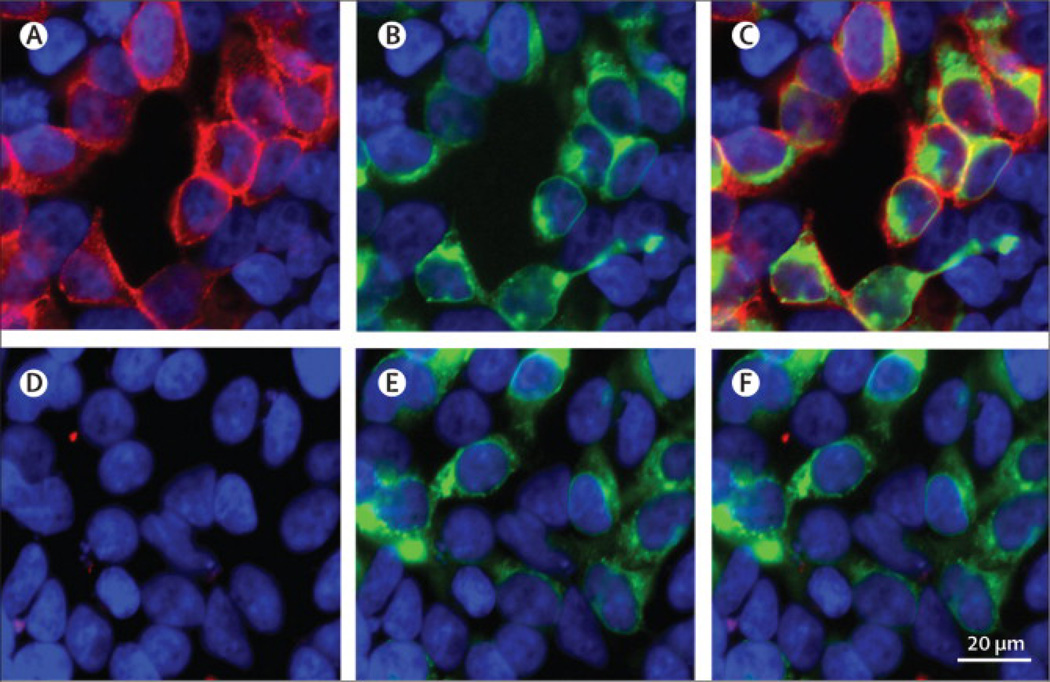
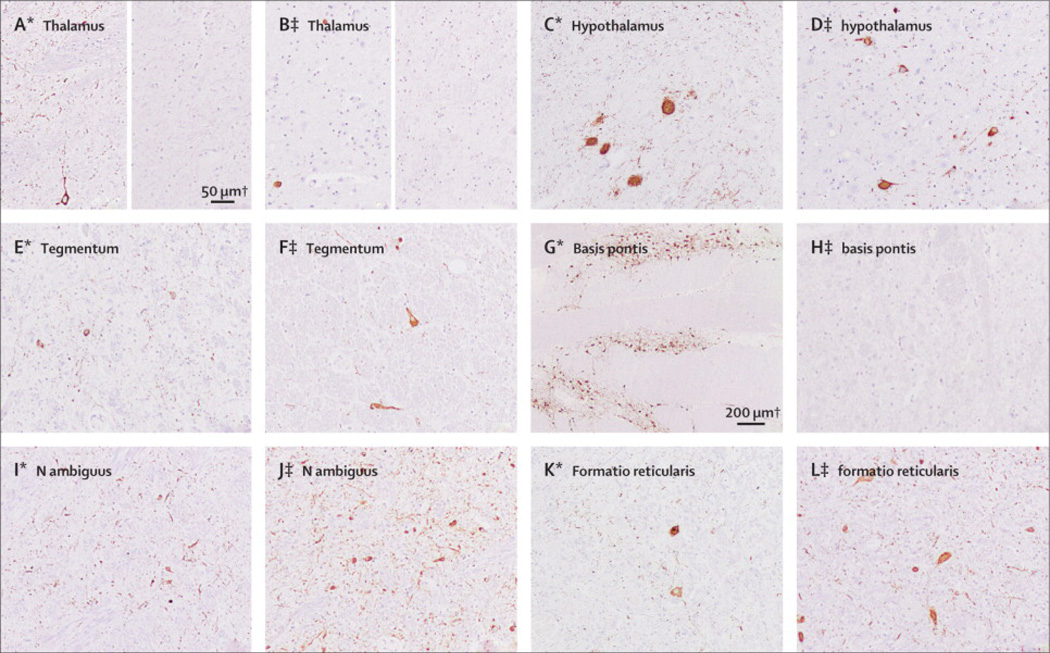
Findings: All eight patients (five women; median age at disease onset 59 years [range 52-76]) had abnormal sleep movements and behaviours and obstructive sleep apnoea, as confirmed by polysomnography. Six patients had chronic progression with a median duration from symptom onset to death or last visit of 5 years (range 2-12); in four the sleep disorder was the initial and most prominent feature, and in two it was preceded by gait instability followed by dysarthria, dysphagia, ataxia, or chorea. Two patients had a rapid progression with disequilibrium, dysarthria, dysphagia, and central hypoventilation, and died 2 months and 6 months, respectively, after symptom onset. In five of five patients, video polysomnography showed features of obstructive sleep apnoea, stridor, and abnormal sleep architecture (undifferentiated non-rapid-eye-movement [non-REM] sleep or poorly structured stage N2, simple movements and finalistic behaviours, normalisation of non-REM sleep by the end of the night, and, in the four patients with REM sleep recorded, REM sleep behaviour disorder). Four of four patients had HLA-DRB1*1001 and HLA-DQB1*0501 alleles. All patients had antibodies (mainly IgG4) against IgLON5, a neuronal cell adhesion molecule. Only one of the 298 controls, who had progressive supranuclear palsy, had IgLON5 antibodies. Neuropathology showed neuronal loss and extensive deposits of hyperphosphorylated tau mainly involving the tegmentum of the brainstem and hypothalamus in the two patients studied.
Interpretation: IgLON5 antibodies identify a unique non-REM and REM parasomnia with sleep breathing dysfunction and pathological features suggesting a tauopathy.
Funding: Fondo de Investigaciones Sanitarias, Centros de Investigación Biomédica en Red de enfermedades neurodegenerativas (CIBERNED) and Respiratorias (CIBERES), Ministerio de Economía y Competitividad, Fundació la Marató TV3, and the National Institutes of Health.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Paralysis lost: a new cause for a common parasomnia?Lancet Neurol. 2014 Jun;13(6):531-2. doi: 10.1016/S1474-4422(14)70099-7. Epub 2014 May 9. Lancet Neurol. 2014. PMID: 24813537 No abstract available.
-
Friend or foe? IgLON5 antibodies in a novel tauopathy with prominent sleep movement disorder, ataxia, and chorea.Mov Disord. 2014 Jul;29(8):989. doi: 10.1002/mds.25926. Epub 2014 May 27. Mov Disord. 2014. PMID: 24865449 No abstract available.
-
Sleep disorder associated with antibodies to IgLON5: parasomnia or agrypnia?-Authors' reply.Lancet Neurol. 2014 Sep;13(9):864-5. doi: 10.1016/S1474-4422(14)70157-7. Lancet Neurol. 2014. PMID: 25142451 No abstract available.
-
Sleep disorder associated with antibodies to IgLON5: parasomnia or agrypnia?Lancet Neurol. 2014 Sep;13(9):864. doi: 10.1016/S1474-4422(14)70127-9. Lancet Neurol. 2014. PMID: 25142452 No abstract available.
References
-
- Cornelius JR, Pittock SJ, McKeon A, et al. Sleep manifestations of voltage-gated potassium channel complex autoimmunity. Arch Neurol. 2011;68:733–738. - PubMed
-
- Iranzo A, Tolosa E, Gelpi E, et al. Neurodegenerative disease status and post-mortem pathology in idiopathic rapid-eye-movement sleep behaviour disorder: an observational cohort study. Lancet Neurol. 2013;12:443–453. - PubMed
-
- Gold M, Pul R, Bach JP, Stangel M, Dodel R. Pathogenic and physiological autoantibodies in the central nervous system. Immunol Rev. 2012;248:68–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
