

Insufficient natriuretic response to continuous intravenous furosemide is associated with poor long-term outcomes in acute decompensated heart failure
- PMID: 24704538
- PMCID: PMC4067259
- DOI: 10.1016/j.cardfail.2014.03.006
Insufficient natriuretic response to continuous intravenous furosemide is associated with poor long-term outcomes in acute decompensated heart failure
Abstract
Background: Treatment of acute decompensated heart failure (ADHF) with loop diuretics, such as furosemide, is frequently complicated by insufficient urine sodium excretion. We hypothesize that insufficient natriuretic response to diuretic therapy, characterized by lower urine sodium (UNa) and urine furosemide, is associated with subsequent inadequate decongestion, worsening renal function, and adverse long term events.
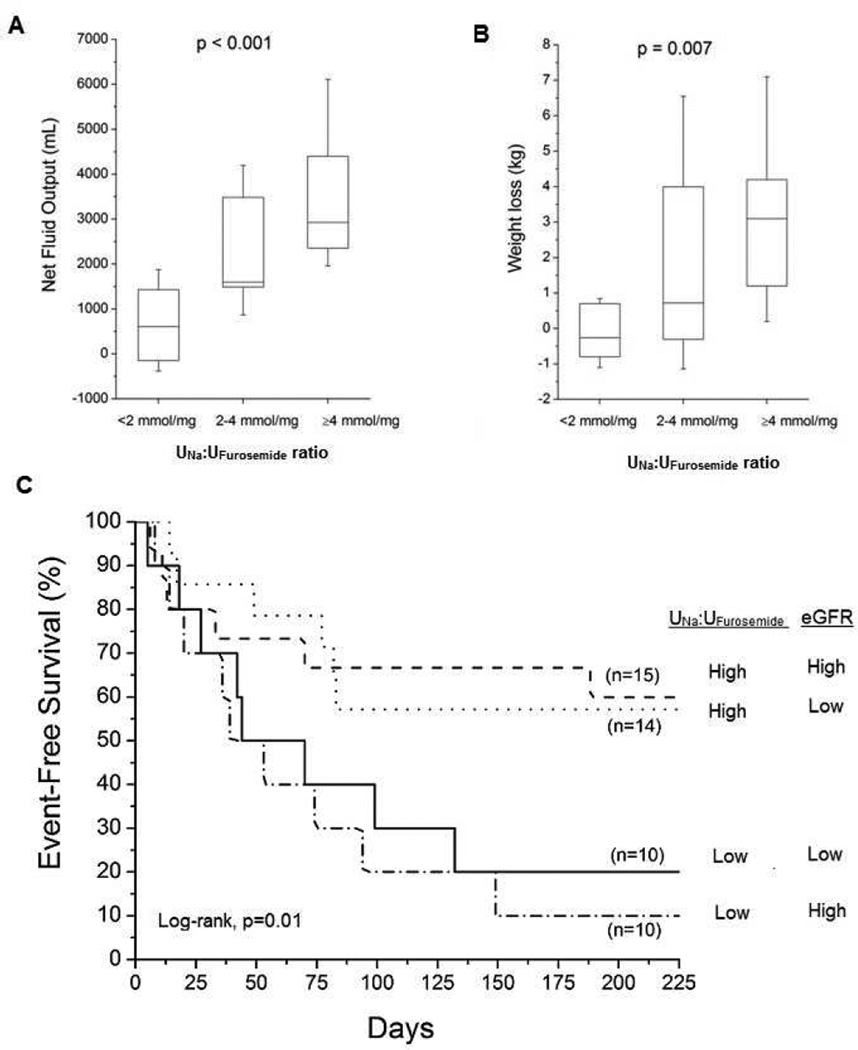
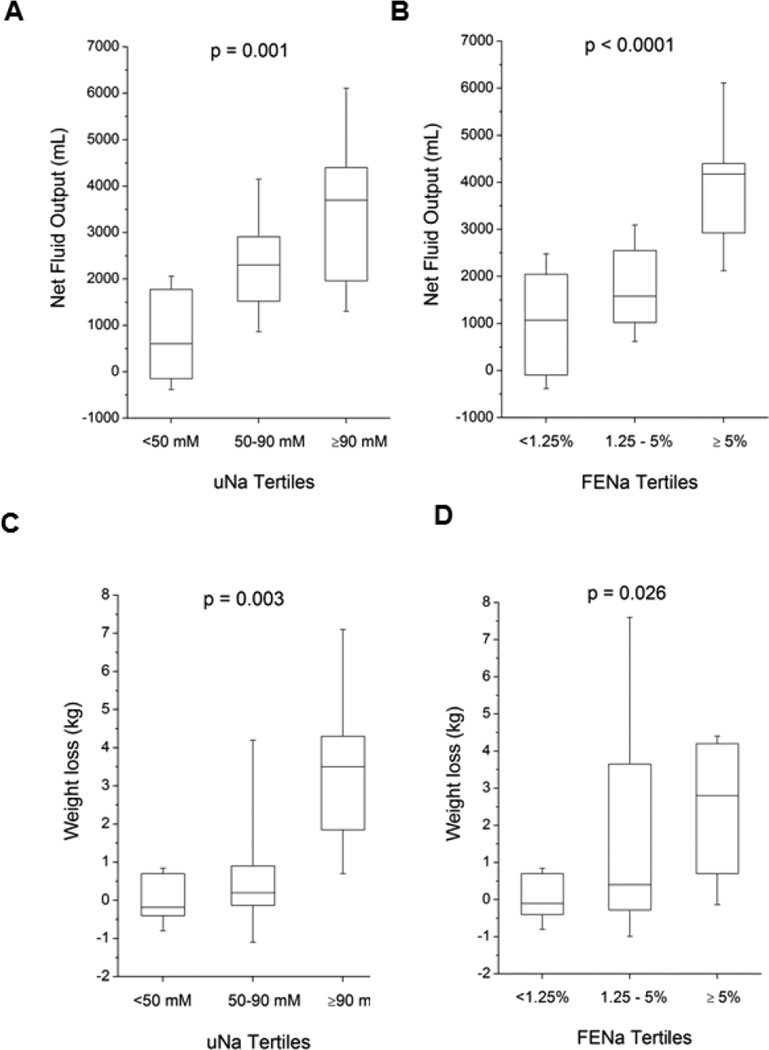
Methods and results: We enrolled 52 consecutive patients with ADHF and measured serum and urine sodium (UNa), urine creatinine (UCr), and urine furosemide (UFurosemide) levels on a spot sample taken after treatment with continuous intravenous furosemide, and followed clinical and renal variables as well as adverse long-term clinical outcomes (death, rehospitalizations, and cardiac transplantation). We observed similar correlations between UNa:UFurosemide ratio and UNa and fractional excretion of sodium (FENa) with 24-hour net urine output (r = 0.52-0.64, all P < .01) and 24-hour weight loss (r = 0.44-0.56; all P < .01). Interestingly, FENa (but not UNa or UNa:UFurosemide) were influenced by estimated glomerular filtration rate (eGFR). We observed an association between lower UNa:UFurosemide with greater likelihood of worsening renal function (hazard ratio [HR] 3.01; P = .02) and poorer adverse clinical outcomes (HR 1.63, P = .008) after adjusting for age and eGFR. Meanwhile, both diminished weight loss and net fluid output over 24 hours of continuous intravenous furosemide were observed when UNa:UFurosemide ratios were <2 mmol/mg or when UNa <50 mmol.
Conclusion: In patients with ADHF receiving continuous furosemide infusion, impaired natriuretic response to furosemide is associated with greater likelihood of worsening renal function and future adverse long-term outcomes, independently from and incrementally with decreasing intrinsic glomerular filtration.
Keywords: Acute decompensated heart failure; furosemide; natriuresis; urine sodium.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, et al. ACCF/AHA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128:1810–1852. 2013. - PubMed
-
- Brater DC. Resistance to loop diuretics. Why it happens and what to do about it. Drugs. 1985;30:427–443. - PubMed
-
- Ellison DH. Diuretic therapy and resistance in congestive heart failure. Cardiology. 2001;96:132–143. - PubMed
-
- Vargo DL, Kramer WG, Black PK, Smith WB, Serpas T, Brater DC. Bioavailability, pharmacokinetics, and pharmacodynamics of torsemide and furosemide in patients with congestive heart failure. Clin Pharmacol Ther. 1995;57:601–609. - PubMed
-
- Brater DC, Chennavasin P, Seiwell R. Furosemide in patients with heart failure: shift in dose-response curves. Clin Pharmacol Ther. 1980;28:182–186. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
