

Recent trends in early stage response to combination antiretroviral therapy in Australia
- PMID: 24704818
- PMCID: PMC4185258
- DOI: 10.3851/IMP2774
Recent trends in early stage response to combination antiretroviral therapy in Australia
Abstract
Background: There have been improvements in combination antiretroviral therapy (cART) over the past 15 years. The aim of this analysis was to assess whether improvements in ART have resulted in improvements in surrogates of HIV outcome.
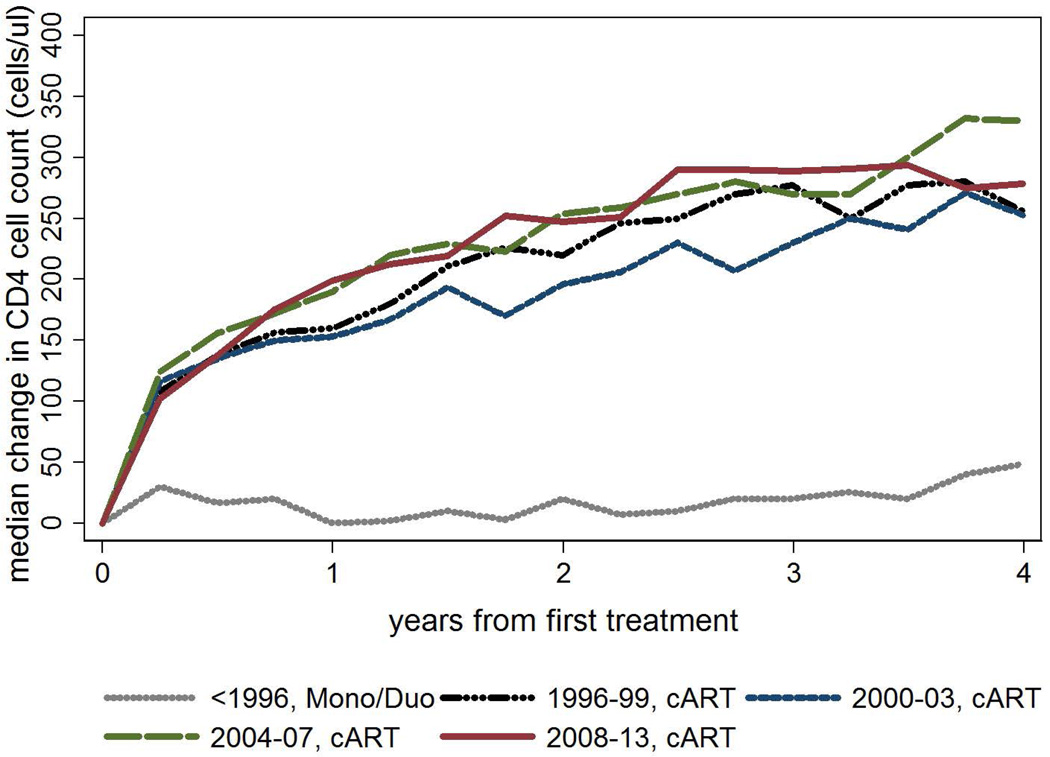
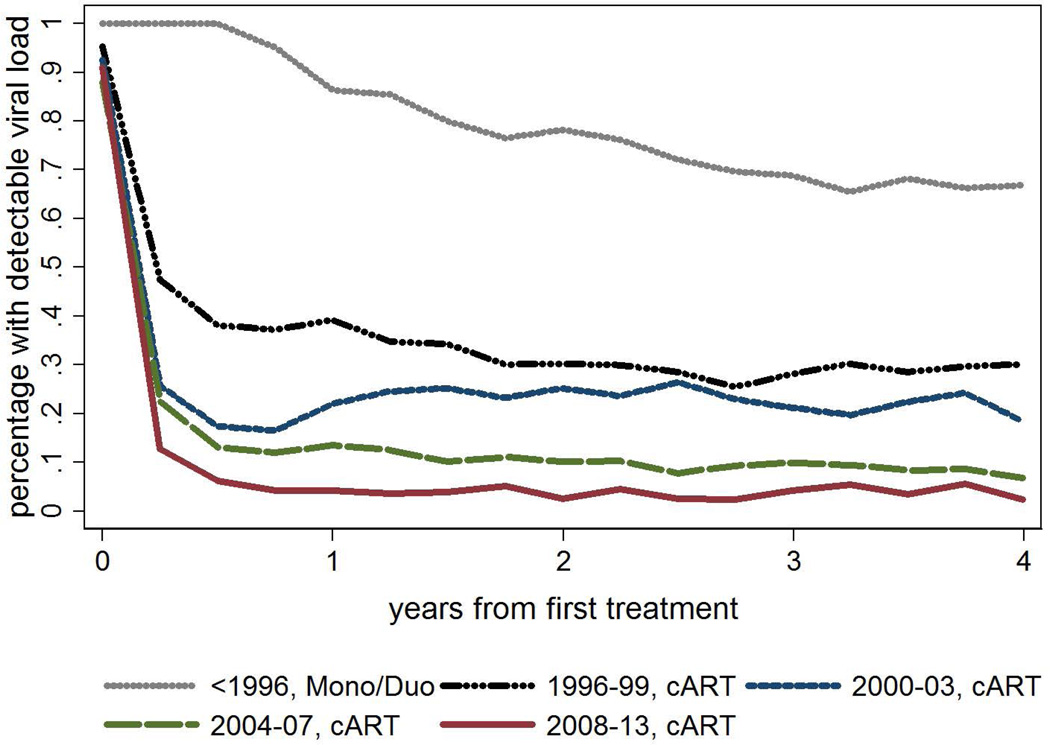
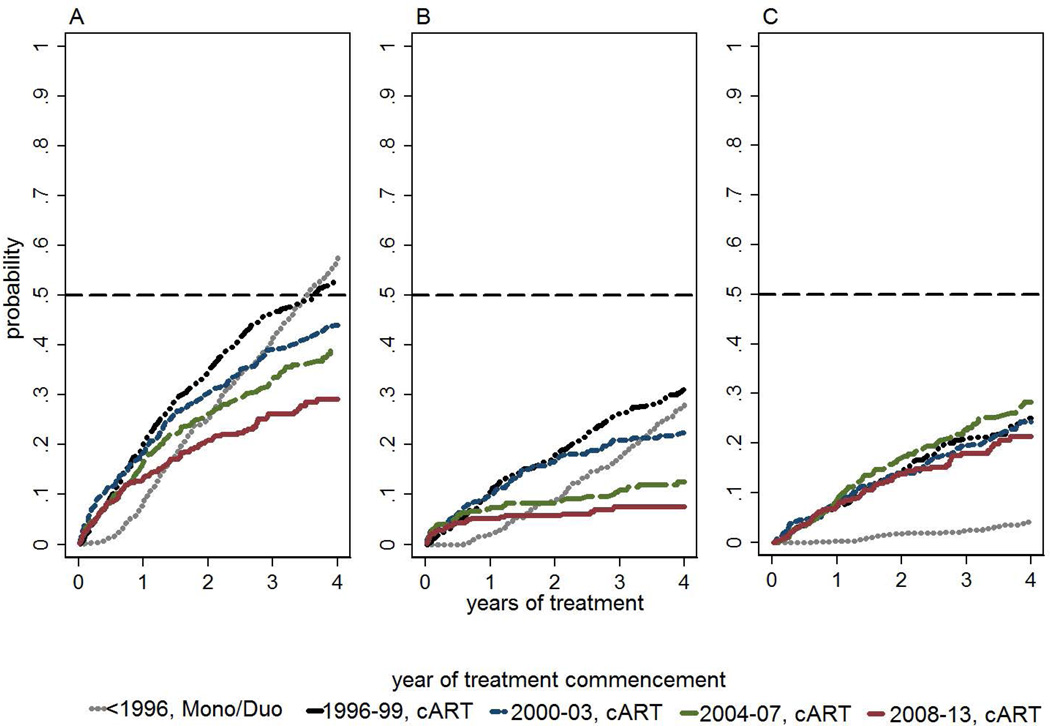
Methods: Patients in the Australian HIV Observational Database who initiated treatment using mono/duo therapy prior to 1996, or using cART from 1996 onwards, were included in the analysis. Patients were stratified by era of ART initiation. Median changes in CD4(+) T-cell count and the proportion of patients with detectable HIV viral load (>400 copies/ml) were calculated over the first 4 years of treatment. Probabilities of treatment switch were estimated using the Kaplan-Meier method.
Results: A total of 2,753 patients were included in the analysis: 28% initiated treatment <1996 using mono/duo therapy and 72% initiated treatment ≥1996 using cART (30% 1996-1999, 12% 2000-2003, 11% 2004-2007 and 19% ≥2008). Overall CD4(+) T-cell count response improved by later era of initiation (P<0.001), although 2000-2003 CD4(+) T-cell count response was less than that for 1996-1999 (P=0.007). The average proportion with detectable viral load from 2 to 4 years post-treatment commencement by era was: <1996 mono/duo 0.69 (0.67-0.71), 1996-1999 cART 0.29 (0.28-0.30), 2000-2003 cART 0.22 (0.20-0.24), 2004-2007 cART 0.09 (0.07-0.10) and ≥2008 cART 0.04 (0.03-0.05). Probability of treatment switch at 4 years after initiation decreased from 53% in 1996-1999 to 29% after 2008 (P<0.001).
Conclusions: Across the five time-periods examined, there have been incremental improvements for patients initiated on cART, as measured by overall response (viral load and CD4(+) T-cell count) and also increased durability of first-line ART regimens.
Figures
References
-
- Boyd MA. Improvements in antiretroviral therapy outcomes over calendar time. Current opinion in HIV and AIDS. 2009;4(3):194–199. Epub 2009/06/18. - PubMed
-
- Llibre JM, Clotet B. Once-daily single-tablet regimens: a long and winding road to excellence in antiretroviral treatment. AIDS reviews. 2012;14(3):168–178. Epub 2012/07/27. - PubMed
-
- Bartlett JA, Fath MJ, Demasi R, Hermes A, Quinn J, Mondou E, et al. An updated systematic overview of triple combination therapy in antiretroviral-naive HIV-infected adults. AIDS. 2006;20(16):2051–2064. Epub 2006/10/21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
