

Proposed morphologic classification of prostate cancer with neuroendocrine differentiation
- PMID: 24705311
- PMCID: PMC4112087
- DOI: 10.1097/PAS.0000000000000208
Proposed morphologic classification of prostate cancer with neuroendocrine differentiation
Abstract
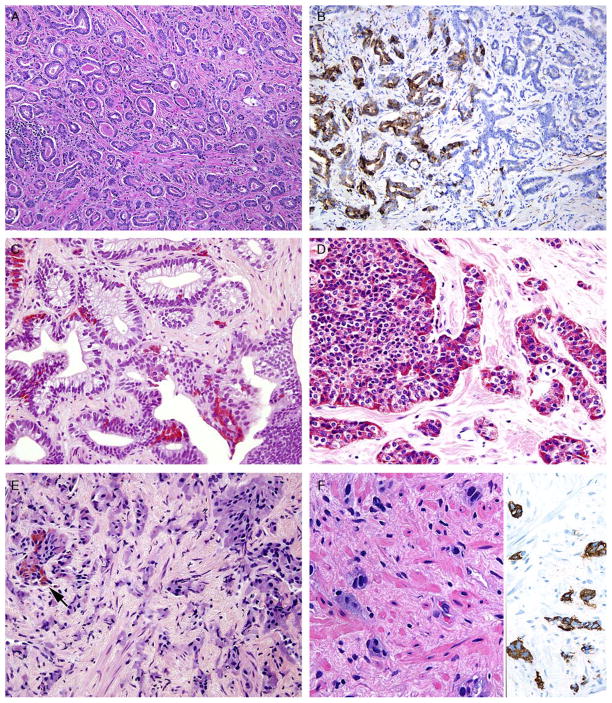
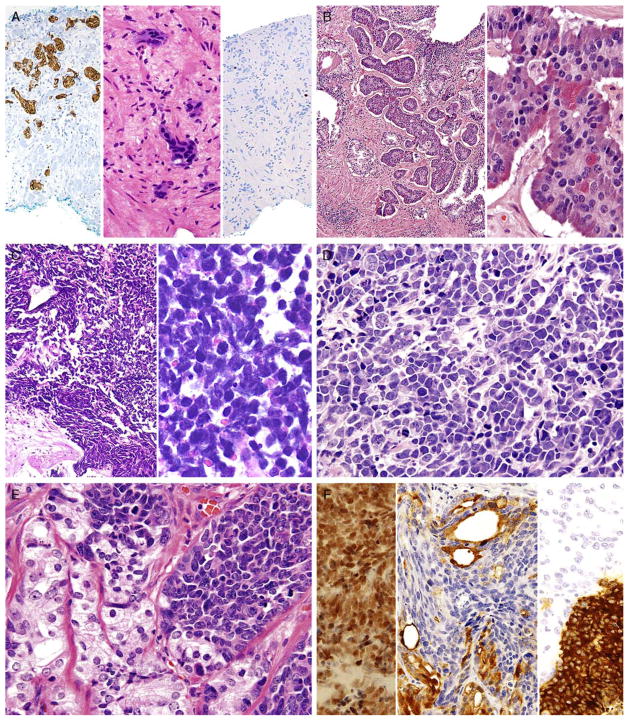
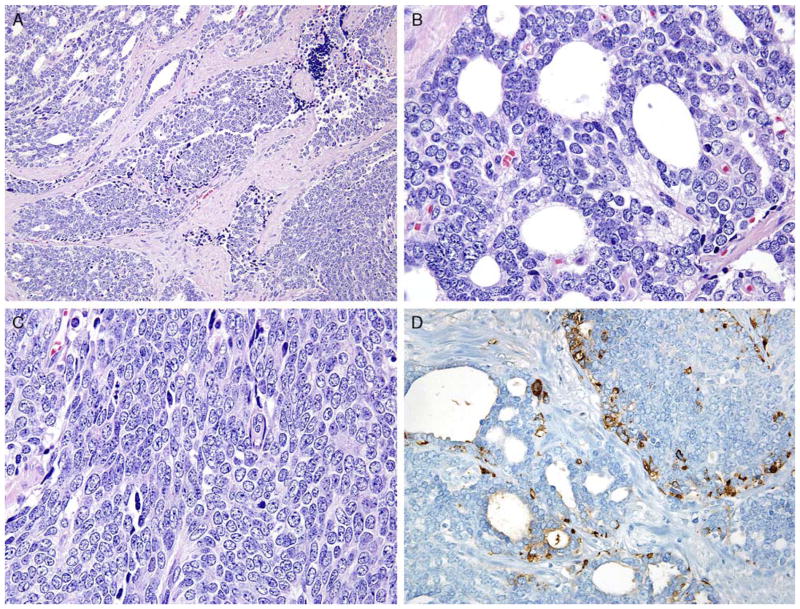
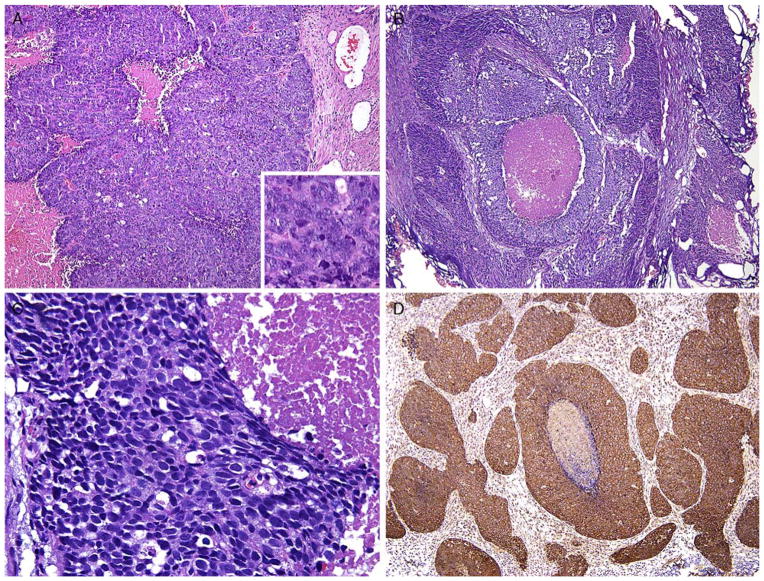
On July 31, 2013, the Prostate Cancer Foundation assembled a working committee on the molecular biology and pathologic classification of neuroendocrine (NE) differentiation in prostate cancer. New clinical and molecular data emerging from prostate cancers treated by contemporary androgen deprivation therapies, as well as primary lesions, have highlighted the need for refinement of diagnostic terminology to encompass the full spectrum of NE differentiation. The classification system consists of: Usual prostate adenocarcinoma with NE differentiation; 2) Adenocarcinoma with Paneth cell NE differentiation; 3) Carcinoid tumor; 4) Small cell carcinoma; 5) Large cell NE carcinoma; and 5) Mixed NE carcinoma - acinar adenocarcinoma. The article also highlights "prostate carcinoma with overlapping features of small cell carcinoma and acinar adenocarcinoma" and "castrate-resistant prostate cancer with small cell cancer-like clinical presentation". It is envisioned that specific criteria associated with the refined diagnostic terminology will lead to clinically relevant pathologic diagnoses that will stimulate further clinical and molecular investigation and identification of appropriate targeted therapies.
Conflict of interest statement
Conflicts of Interest and Source of Funding: The authors have disclosed that they have no significant relationships with, or financial interest in, any commercial companies pertaining to this article.
Figures
References
-
- Abrahamsson PA. Neuroendocrine cells in tumour growth of the prostate. Endocr Relat Cancer. 1999;6:503–519. - PubMed
-
- Abrahamsson PA, Wadstrom LB, Alumets J, et al. Peptidehormone- and serotonin-immunoreactive tumour cells in carcinoma of the prostate. Pathol Res Pract. 1987;182:298–307. - PubMed
-
- Bonkhoff H, Stein U, Remberger K. Androgen receptor status in endocrine-paracrine cell types of the normal, hyperplastic, and neoplastic human prostate. Virchows Arch A Pathol Anat Histopathol. 1993;423:291–294. - PubMed
-
- Azzopardi JG, Evans DJ. Argentaffin cells in prostatic carcinoma: differentiation from lipofuscin and melanin in prostatic epithelium. J Pathol. 1971;104:247–251. - PubMed
-
- Kazzaz BA. Argentaffin and argyrophil cells in the prostate. J Pathol. 1974;112:189–193. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
