

Clinicopathologic characterization of diffuse-large-B-cell lymphoma with an associated serum monoclonal IgM component
- PMID: 24705344
- PMCID: PMC3976325
- DOI: 10.1371/journal.pone.0093903
Clinicopathologic characterization of diffuse-large-B-cell lymphoma with an associated serum monoclonal IgM component
Abstract
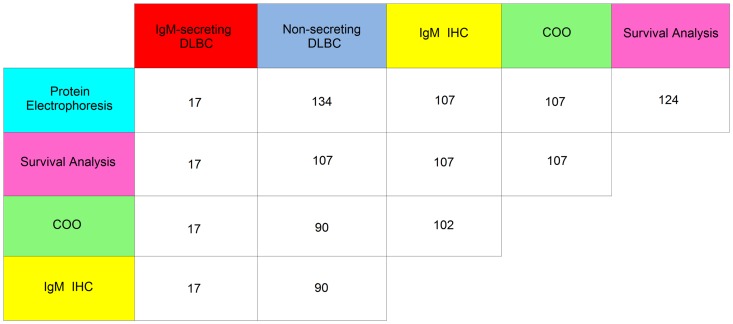
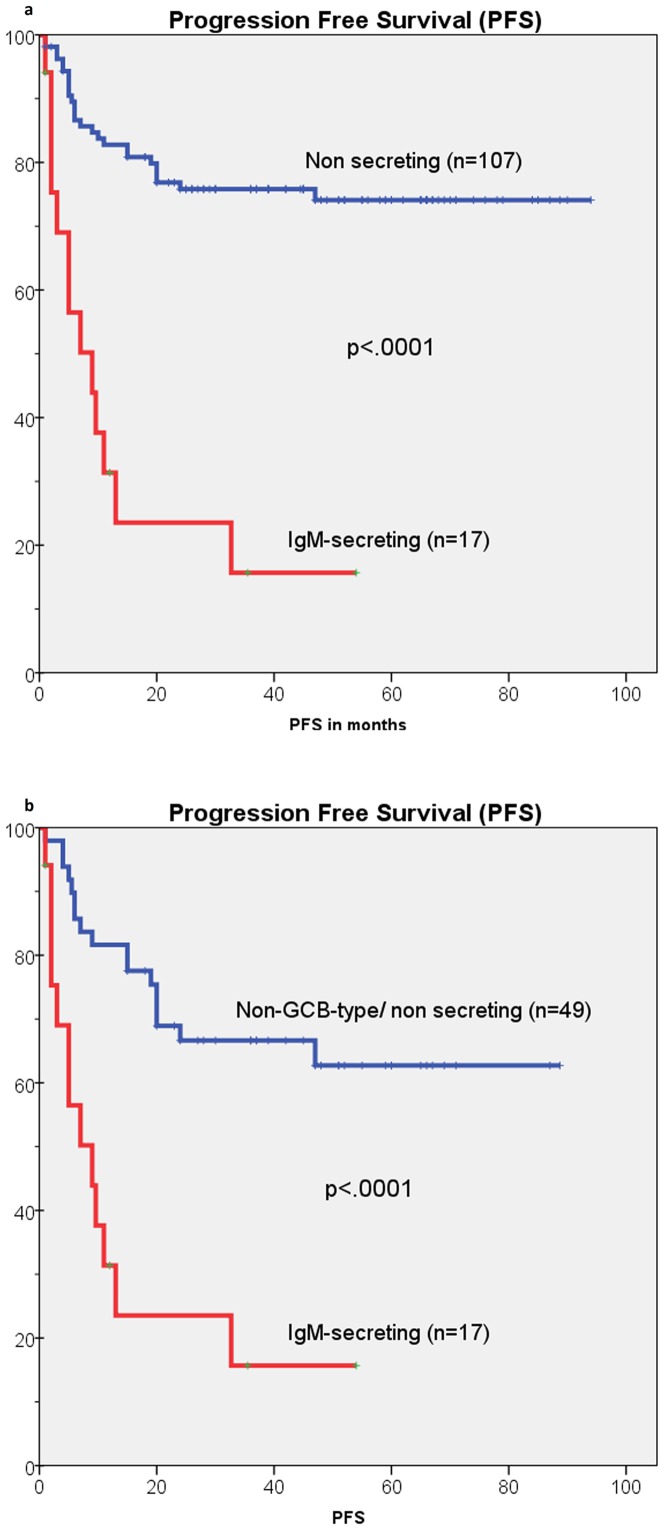
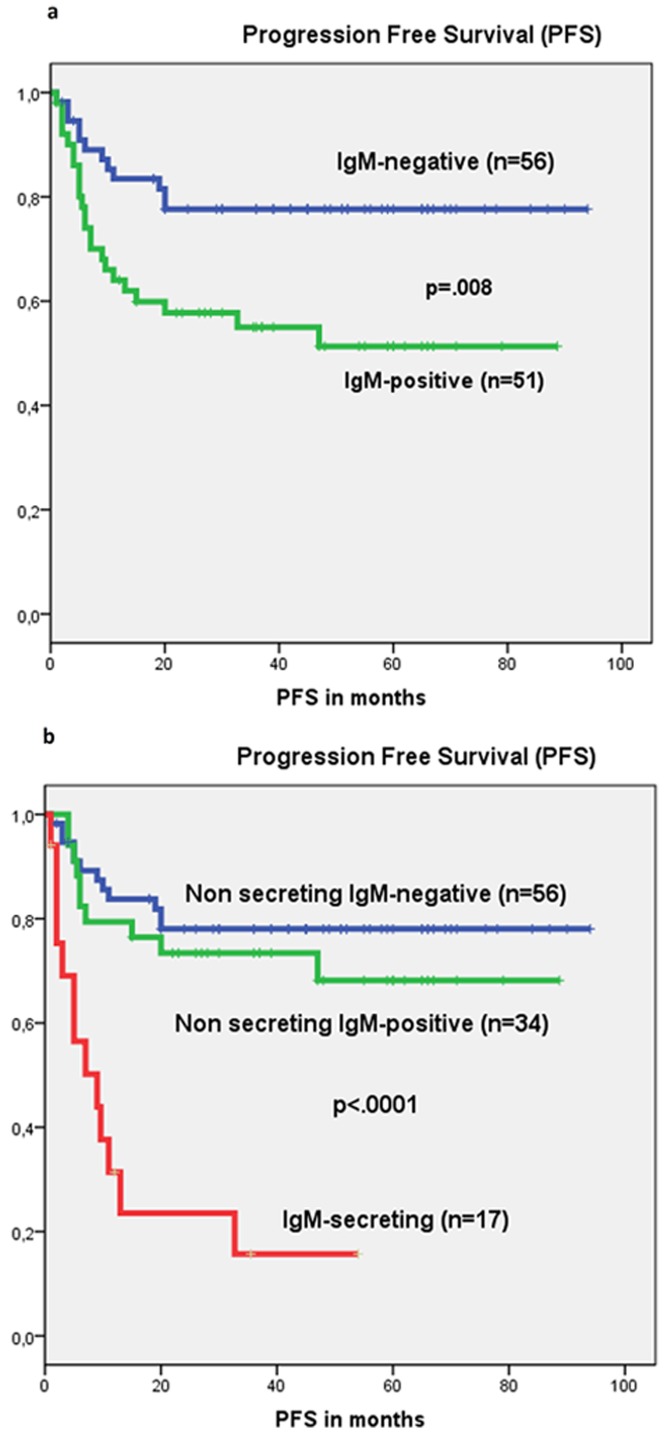
Recently, diffuse-large-B-cell lymphoma (DLBCL) associated with serum IgM monoclonal component (MC) has been shown to be a very poor prognostic subset although, detailed pathological and molecular data are still lacking. In the present study, the clinicopathological features and survival of IgM-secreting DLBCL were analyzed and compared to non-secreting cases in a series of 151 conventional DLBCL treated with R-CHOP. IgM MC was detected in 19 (12.5%) out of 151 patients at disease onset. In 17 of these cases secretion was likely due to the neoplastic clone, as suggested by the expression of heavy chain IgM protein in the cytoplasm of tumor cells. In IgM-secreting cases immunoblastic features (p<.0001), non-GCB-type (p = .002) stage III-IV(p = .003), ≥ 2 extra nodal sites (p<.0001), bone-marrow (p = .002), central-nervous-system (CNS) involvement at disease onset or relapse (p<.0001), IPI-score 3-5 (p = .009) and failure to achieve complete remission (p = .005), were significantly more frequent. FISH analyses for BCL2, BCL6 and MYC gene rearrangements detected only two cases harboring BCL2 gene translocation and in one case a concomitant BCL6 gene translocation was also observed. None of the IgM-secreting DLBCL was found to have L265P mutation of MYD88 gene. Thirty-six month event-free (11.8% vs 66.4% p<.0001), progression-free (23.5% vs 75.7%, p<.0001) and overall (47.1% vs 74.8%, p<.0001) survivals were significantly worse in the IgM-secreting group. In multivariate analysis IgM-secreting (p = .005, expB = 0.339, CI = 0.160-0.716) and IPI-score 3-5 (p = .010, expB = 0.274, CI = 0.102-0.737) were the only significant factors for progression-free-survival. Notably, four relapsed patients, who were treated with salvage immunochemotherapy combined with bortezomib or lenalidomide, achieved lasting remission. Our data suggests that IgM-secreting cases are a distinct subset of DLBCL, originating from activated-B-cells with terminally differentiated features, prevalent extra nodal dissemination and at high risk of CNS involvement.
Conflict of interest statement
Figures
References
-
- Fu K, Weisenburger DD, Choi WW, Perry KD, Smith LM, et al. (2008) Addition of rituximab to standard chemotherapy improves the survival of both the germinal center B-cell-like and non-germinal center B-cell-like subtypes of diffuse large B-cell lymphoma. J Clin Oncol 2628: 4587–94. - PubMed
-
- Sehn LH, DJ, Chanabhai M, Fitzgerald C, Gill K, Klasa R, et al. (2005) Introduction of combined CHOP plus rituximab therapy dramatically improved outcome of diffuse large B-cell lymphoma in British Columbia. J ClinOncol 23: 5027–5033. - PubMed
-
- Project, TIN-HsLPF (1993) A predictive model for aggressive non-Hodgkin's lymphoma The International Non-Hodgkin's Lymphoma Prognostic Factors Project. N Engl J Med 329: 987–994. - PubMed
-
- Alizadeh AA, Davis EM, Ma RE, Lossos C, Rosenwald A, et al. (2000) Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature 3 403: 503–511. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
