

Burden of hospital admission and repeat angiography in angina pectoris patients with and without coronary artery disease: a registry-based cohort study
- PMID: 24705387
- PMCID: PMC3976412
- DOI: 10.1371/journal.pone.0093170
Burden of hospital admission and repeat angiography in angina pectoris patients with and without coronary artery disease: a registry-based cohort study
Abstract
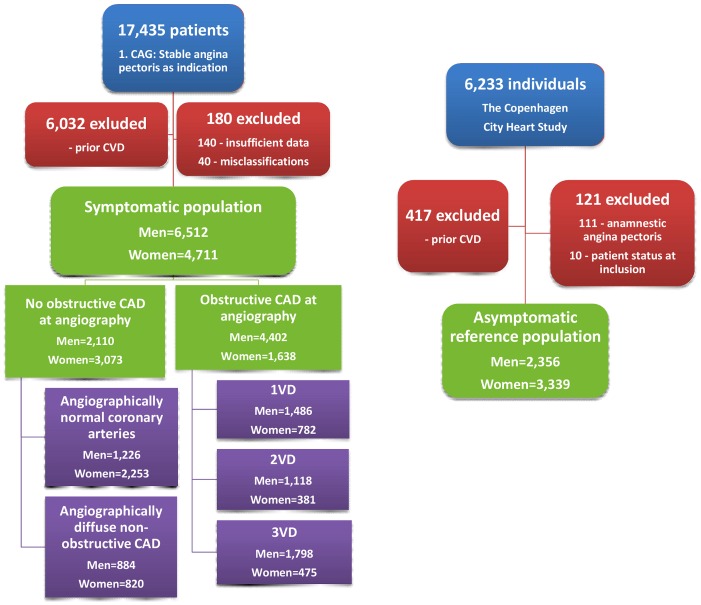
Aims: To evaluate risk of hospitalization due to cardiovascular disease (CVD) and repeat coronary angiography (CAG) in stable angina pectoris (SAP) with no obstructive coronary artery disease (CAD) versus obstructive CAD, and asymptomatic reference individuals.
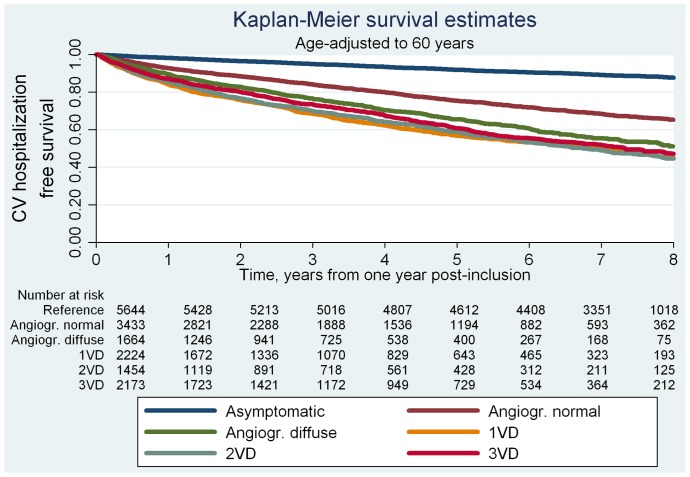
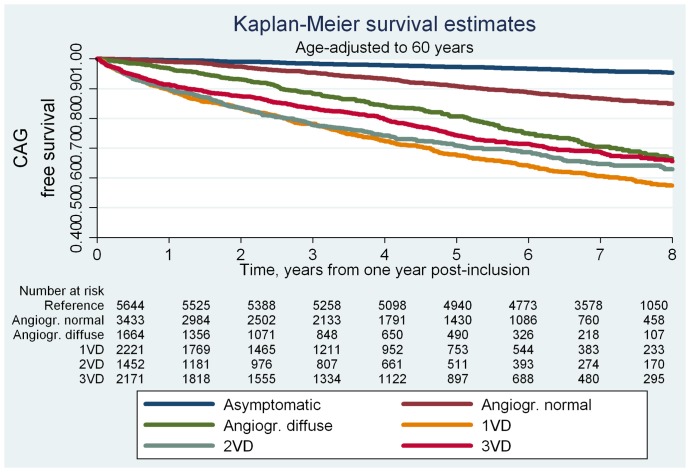
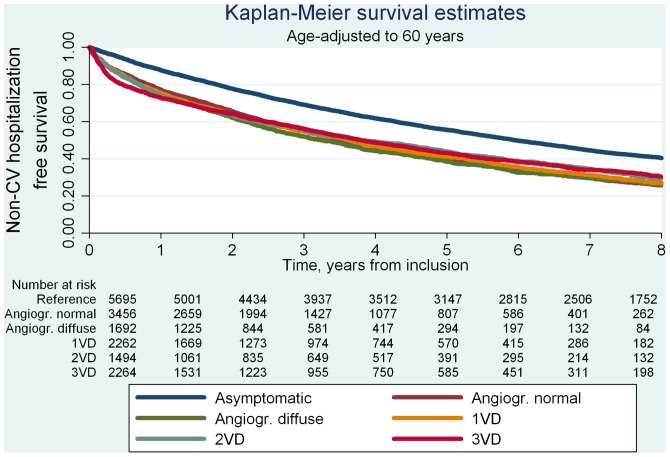
Methods and results: We followed 11,223 patients with no prior CVD having a first-time CAG in 1998-2009 due to SAP symptoms and 5,695 asymptomatic reference individuals from the Copenhagen City Heart Study through registry linkage for 7.8 years (median). In recurrent event survival analysis, patients with SAP had 3-4-fold higher risk of hospitalization for CVD irrespective of CAG findings and cardiovascular comorbidity. Multivariable adjusted hazard ratios(95%CI) for patients with angiographically normal coronary arteries was 3.0(2.5-3.5), for angiographically diffuse non-obstructive CAD 3.9(3.3-4.6) and for 1-3-vessel disease 3.6-4.1(range)(all P<0.001). Mean accumulated hospitalization time was 3.5(3.0-4.0)(days/10 years follow-up) in reference individuals and 4.5(3.8-5.2)/7.0(5.4-8.6)/6.7(5.2-8.1)/6.1(5.2-7.4)/8.6(6.6-10.7) in patients with angiographically normal coronary arteries/angiographically diffuse non-obstructive CAD/1-, 2-, and 3-vessel disease, respectively (all P<0.05, age-adjusted). SAP symptoms predicted repeat CAG with multivariable adjusted hazard ratios for patients with angiographically normal coronary arteries being 2.3(1.9-2.9), for angiographically diffuse non-obstructive CAD 5.5(4.4-6.8) and for obstructive CAD 6.6-9.4(range)(all P<0.001).
Conclusions: Patients with SAP symptoms and angiographically normal coronary arteries or angiographically diffuse non-obstructive CAD suffer from considerably greater CVD burdens in terms of hospitalization for CVD and repeat CAG compared with asymptomatic reference individuals even after adjustment for cardiac risk factors and exclusion of cardiovascular comorbidity as cause. Contrary to common perception, excluding obstructive CAD by CAG in such patients does not ensure a benign cardiovascular prognosis.
Conflict of interest statement
Figures
References
-
- Jespersen L, Hvelplund A, Abildstrom SZ, Pedersen F, Galatius S, et al. (2012) Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. European Heart Journal 33: 734–744. - PubMed
-
- Jespersen L, Abildstrom SZ, Hvelplund A, Prescott E (2013) Persistent angina: highly prevalent and associated with long-term anxiety, depression, low physical functioning, and quality of life in stable angina pectoris. Clin Res Cardiol 102: 571–581. - PubMed
-
- Shaw LJ, Merz CNB, Pepine CJ, Reis SE, Bittner V, et al. (2006) The Economic Burden of Angina in Women With Suspected Ischemic Heart Disease: Results From the National Institutes of Health-National Heart, Lung, and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation. Circulation 114: 894–904. - PubMed
-
- Schnohr P, Jensen GB, Lange P, Scharling H, Appleyard M (2001) The Copenhagen City heart study - Introduction. European Heart Journal Supplements 3: H1–H83.
-
- Hemingway H, Vahtera J, Virtanen M, Pentti J, Kivimäki M (2007) Outcome of stable angina in a working population: the burden of sickness absence. European Journal of Cardiovascular Prevention & Rehabilitation 14: 373–379. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
