

Low birth weight in perinatally HIV-exposed uninfected infants: observations in urban settings in Cameroon
- PMID: 24705410
- PMCID: PMC3976419
- DOI: 10.1371/journal.pone.0093554
Low birth weight in perinatally HIV-exposed uninfected infants: observations in urban settings in Cameroon
Abstract
Background: The consequences of maternal HIV infection for fetal growth are controversial. Here, we estimated the frequency of small for gestational age and gender (SGAG) among neonates born to HIV-infected or uninfected mothers and assessed the contribution, if any, of maternal HIV to the risk of SGAG.
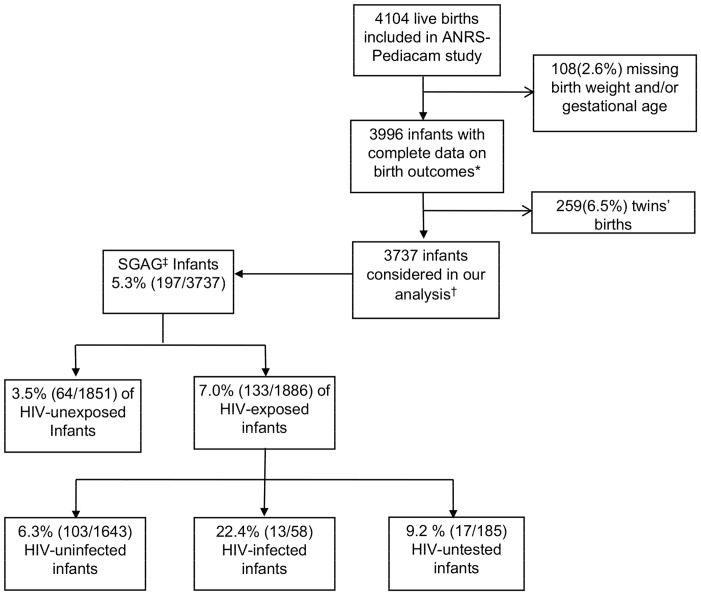
Methods: The data used were obtained from the ANRS-Pediacam cohort in Cameroon. Pairs of newborns, one to a HIV-infected mother and the other to an uninfected mother, were identified during the first week of life, and matched on gender and recruitment site from 2007-2010. SGAG was defined in line with international recommendations as a birth weight Z-score adjusted for gestational age at delivery and gender more than two standard deviations below the mean (-2SD). Considering the matched design, logistic regression modeling was adjusted on site and gender to explore the effect of perinatal HIV exposure on SGAG.
Results: Among the 4104 mother-infant pairs originally enrolled, no data on birth weight and/or gestational age were available for 108; also, 259 were twins and were excluded. Of the remaining 3737 mother-infant pairs, the frequency of SGAG was 5.3% (95%CI: 4.6-6.0), and was significantly higher among HIV-infected infants (22.4% vs. 6.3%; p<.001) and lower among HIV-unexposed uninfected infants (3.5% vs. 6.3%; p<.001) than among HIV-exposed uninfected infants. Similarly, SGAG was significantly more frequent among HIV-infected infants (aOR: 4.1; 2.0-8.1) and less frequent among HIV-unexposed uninfected infants (aOR: 0.5; 0.4-0.8) than among HIV-exposed uninfected infants. Primiparity (aOR: 1.9; 1.3-2.7) and the presence of any disease during pregnancy (aOR: 1.4; 1.0-2.0) were identified as other contributors to SGAG.
Conclusion: Maternal HIV infection was independently associated with SGAG for HIV-exposed uninfected infants. This provides further evidence of the need for adapted monitoring of pregnancy in HIV-infected women, especially if they are symptomatic, to minimize additional risk factors for SGAG.
Conflict of interest statement
Figures
References
-
- Bailey RC, Kamenga MC, Nsuami MJ, Nieburg P, St Louis ME (1999) Growth of children according to maternal and child HIV, immunological and disease characteristics: a prospective cohort study in Kinshasa, Democratic Republic of Congo. Int J Epidemiol 28: 532–40. - PubMed
-
- Dreyfuss ML, Msamanga GI, Spiegelman D, Hunter DJ, Urassa EJ, et al. (2001) Determinants of low birth weight among HIV-infected pregnant women in Tanzania. Am J Clin Nutr 74: 814–26. - PubMed
-
- Lepage P, Msellati P, Hitimana DG, Bazubagira A, Van Goethem C, et al. (1996) Growth of human immunodeficiency type 1-infected and uninfected children: a prospective cohort study in Kigali, Rwanda, 1988 to 1993. Pediatr Infect Dis J 15: 479–85. - PubMed
-
- Makasa M, Kasonka L, Chisenga M, Sinkala M, Chintu C, et al. (2007) Early growth of infants of HIV-infected and uninfected Zambian women. Trop Med Int Health 12: 594–602. - PubMed
-
- Marinda E, Humphrey JH, Iliff PJ, Mutasa K, Nathoo KJ, et al. (2007) Child mortality according to maternal and infant HIV status in Zimbabwe. Pediatr Infect Dis J 26: 519–26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
