

Associations between antidepressant adherence and shared decision-making, patient-provider trust, and communication among adults with diabetes: diabetes study of Northern California (DISTANCE)
- PMID: 24706097
- PMCID: PMC4099457
- DOI: 10.1007/s11606-014-2845-6
Associations between antidepressant adherence and shared decision-making, patient-provider trust, and communication among adults with diabetes: diabetes study of Northern California (DISTANCE)
Abstract
Background: Depression and adherence to antidepressant treatment are important clinical concerns in diabetes care. While patient-provider communication patterns have been associated with adherence for cardiometabolic medications, it is unknown whether interpersonal aspects of care impact antidepressant medication adherence.
Objective: To determine whether shared decision-making, patient-provider trust, or communication are associated with early stage and ongoing antidepressant adherence.
Design: Observational new prescription cohort study.
Setting: Kaiser Permanente Northern California.
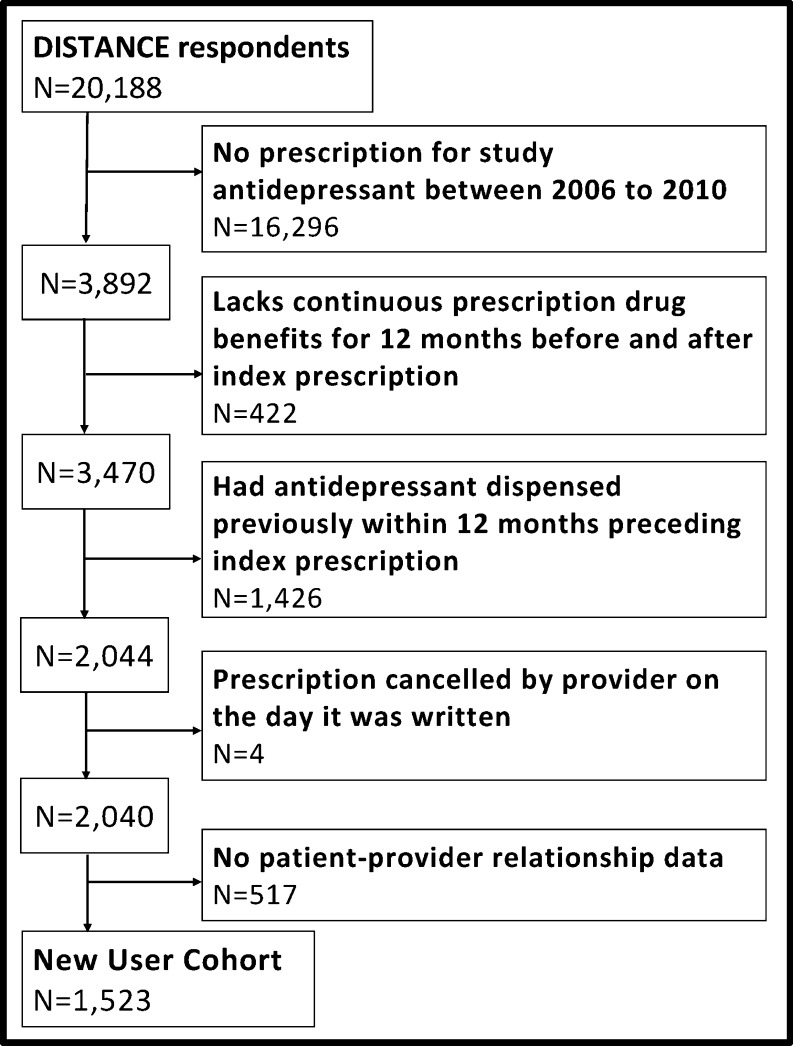
Patients: One thousand five hundred twenty-three adults with type 2 diabetes who completed a survey in 2006 and received a new antidepressant prescription during 2006-2010.
Measurements: Exposures included items based on the Trust in Physicians and Interpersonal Processes of Care instruments and the Consumer Assessment of Healthcare Providers and Systems (CAHPS) communication scale. Measures of adherence were estimated using validated methods with physician prescribing and pharmacy dispensing data: primary non-adherence (medication never dispensed), early non-persistence (dispensed once, never refilled), and new prescription medication gap (NPMG; proportion of time without medication during 12 months after initial prescription).
Results: After adjusting for potential confounders, patients' perceived lack of shared decision-making was significantly associated with primary non-adherence (RR = 2.42, p < 0.05), early non-persistence (RR = 1.34, p < 0.01) and NPMG (estimated 5% greater gap in medication supply, p < 0.01). Less trust in provider was significantly associated with early non-persistence (RRs 1.22-1.25, ps < 0.05) and NPMG (estimated NPMG differences 5-8%, ps < 0.01).
Limitations: All patients were insured and had consistent access to and quality of care.
Conclusions: Patients' perceptions of their relationships with providers, including lack of shared decision-making or trust, demonstrated strong associations with antidepressant non-adherence. Further research should explore whether interventions for healthcare providers and systems that foster shared decision-making and trust might also improve medication adherence.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
