

Multi-slice computed tomography assessment of bronchial compression with absent pulmonary valve
- PMID: 24706163
- PMCID: PMC4061480
- DOI: 10.1007/s00247-014-2898-z
Multi-slice computed tomography assessment of bronchial compression with absent pulmonary valve
Abstract
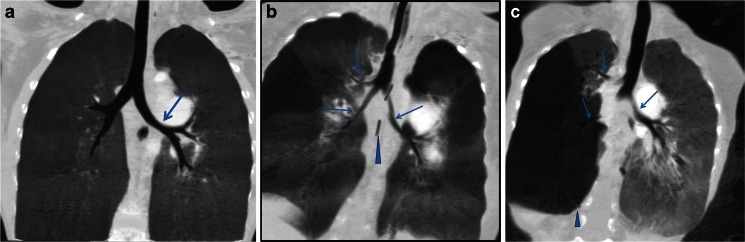
Background: Absent pulmonary valve is a rare cardiovascular anomaly that can result in profound tracheobronchial compression.
Objective: To demonstrate the advantage of multi-slice CT in diagnosing tracheobronchial compression, its severity as related to the adjacent dilated pulmonary arteries, and associated lung and cardiac lesions.
Materials and methods: We included children with absent pulmonary valve who were reviewed by multi-slice CT during a 17-year period. The number and locations of stenoses and lung lesions were noted and the severity of stenosis was categorized. The diameter of the pulmonary artery was measured and associated cardiac defects were demonstrated.
Results: Thirty-one children (14 girls and 17 boys) were included. Of these, 29 had ventricular septal defect and 2 had an intact ventricular septum. Twenty-nine children (94%) had tracheobronchial compression, judged to be mild in nine children (31%), moderate in 10 (34%) and severe in 10 (34%). The different locations of the stenosis (carina, main bronchi, lobar and segmental bronchi) were observed. And the number and location of lung lesions demonstrated that the right middle and left upper and lower lobes were often affected. The diameter of the pulmonary artery in these children was well above normal published values, and Spearman rank correlation analysis showed a correlation between the size of the pulmonary artery and the severity of the tracheobronchial stenosis. Nineteen children (61%) underwent surgery and 4 of these children had a multi-slice CT post-operative follow-up study.
Conclusion: Absent pulmonary valve can cause significant morbidity and mortality in children. Multi-slice CT can accurately depict areas of tracheobronchial compression, associated lung lesions and cardiac defects, helping to direct the surgeon.
Figures



Similar articles
-
Combined Surgical and Endoscopic Approach for Ring-Sling Complex.Thorac Cardiovasc Surg. 2020 Jan;68(1):51-58. doi: 10.1055/s-0039-1678670. Epub 2019 Feb 11. Thorac Cardiovasc Surg. 2020. PMID: 30743276
-
Tracheobronchial compression in acyanotic congenital heart disease.Ann Otol Rhinol Laryngol. 1983 Jul-Aug;92(4 Pt 1):387-90. doi: 10.1177/000348948309200419. Ann Otol Rhinol Laryngol. 1983. PMID: 6881845
-
The Lecompte maneuver for relief of airway compression in absent pulmonary valve syndrome.Ann Thorac Surg. 2006 May;81(5):1802-7. doi: 10.1016/j.athoracsur.2005.12.001. Ann Thorac Surg. 2006. PMID: 16631676
-
Compression of adjacent anatomical structures by pulmonary artery dilation.Postgrad Med. 2016 Jun;128(5):451-9. doi: 10.1080/00325481.2016.1157442. Epub 2016 Mar 7. Postgrad Med. 2016. PMID: 26898826 Free PMC article. Review.
-
Congenital avalvular pulmonary artery and infantile lobar emphysema. A diagnostic correlation.Am J Roentgenol Radium Ther Nucl Med. 1975 Oct;125(2):412-21. doi: 10.2214/ajr.125.2.412. Am J Roentgenol Radium Ther Nucl Med. 1975. PMID: 1106224 Review.
Cited by
-
Pediatric Cardiothoracic CT Guideline Provided by the Asian Society of Cardiovascular Imaging Congenital Heart Disease Study Group: Part 2. Contemporary Clinical Applications.Korean J Radiol. 2021 Aug;22(8):1397-1415. doi: 10.3348/kjr.2020.1332. Epub 2021 May 4. Korean J Radiol. 2021. PMID: 33987995 Free PMC article. Review.
-
Computed tomography in tetralogy of Fallot: pre- and postoperative imaging evaluation.Pediatr Radiol. 2022 Dec;52(13):2485-2497. doi: 10.1007/s00247-021-05179-5. Epub 2021 Aug 24. Pediatr Radiol. 2022. PMID: 34427695 Review.
References
-
- Freedom RM, Mawson JB, Yoo SJ, et al. Congenital heart disease: textbook of angiography. New York: Futura Publishing Co.; 1997. pp. 597–615.
-
- Quint LE, Whyte RI, Kazerooni EA, et al. Stenosis of the central airways: evaluation by using helical CT with multiplanar reconstructions. Radiology. 1995;194:871–877. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
